See other “How to”
Cold snare polypectomy
Description :
Cold snare polypectomy is now the technique of choice for resection of polyps up to 10 mm in size, as it eliminates the risk of perforation and delayed bleeding, and visual feedback allows real-time assessment of immediate bleeding.
Before the procedure:
- Make sure everything is all set in the exam room
- Take care of the patient, monitor him throughout the procedure
- Hygiene is an essential issue, both for the patient and for the staff
- Wash your hands often, wear gloves, mask and goggles, protective equipment, comply with universal precautions
- And, of course, good cooperation between doctor and nurse contributes to a successful procedure.
Cold snare polypectomy is usually performed with a small snare, with an opening diameter of 9 to 15 mm, but there is not enough evidence that larger snares, of 20, 25, 35 mm, would not be effective. The frequent recommendation is that the sanres used for cold polypectomy have a thin thread (monofilament), of 0.3 mm, because our experience has proven that these threads can achieve a more effective resection, compared to standard snares (braided or multifilament), with 0.4/0.48 mm in wire diameter.
There are snares specially designed for cold polypectomy, with oval, hexagonal, rhomboidal loop shape that can more effectively surround small or diminutive lesions and achieve a clear margin of normal tissue. Cold polypectomy snares are made of a stronger and therefore much stiffer material, which prevents the catheter from fracturing when the snare is closed. Traditional snares have softer catheters that usually close upon complete closure of the snare thread without tissue transition.
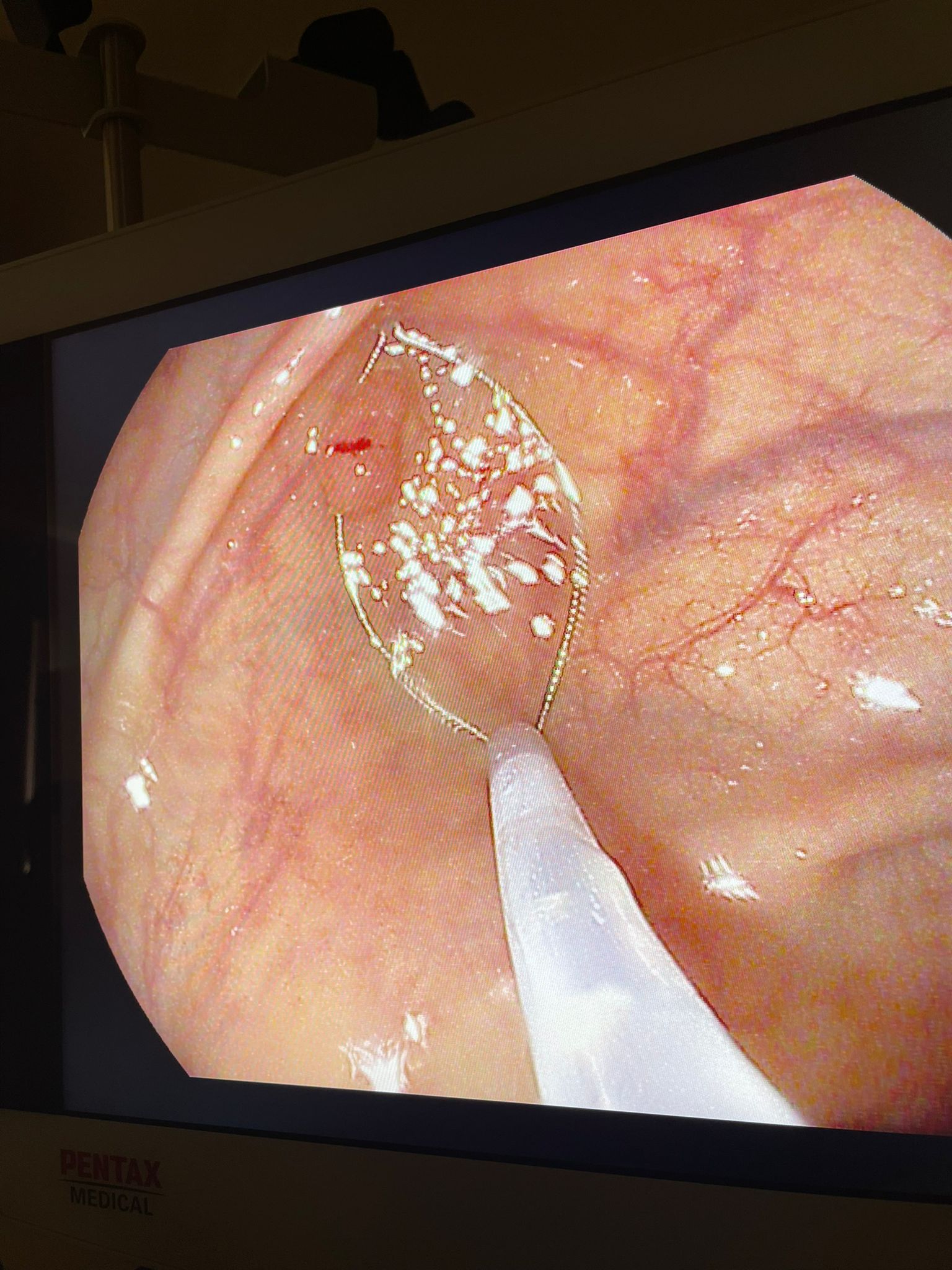
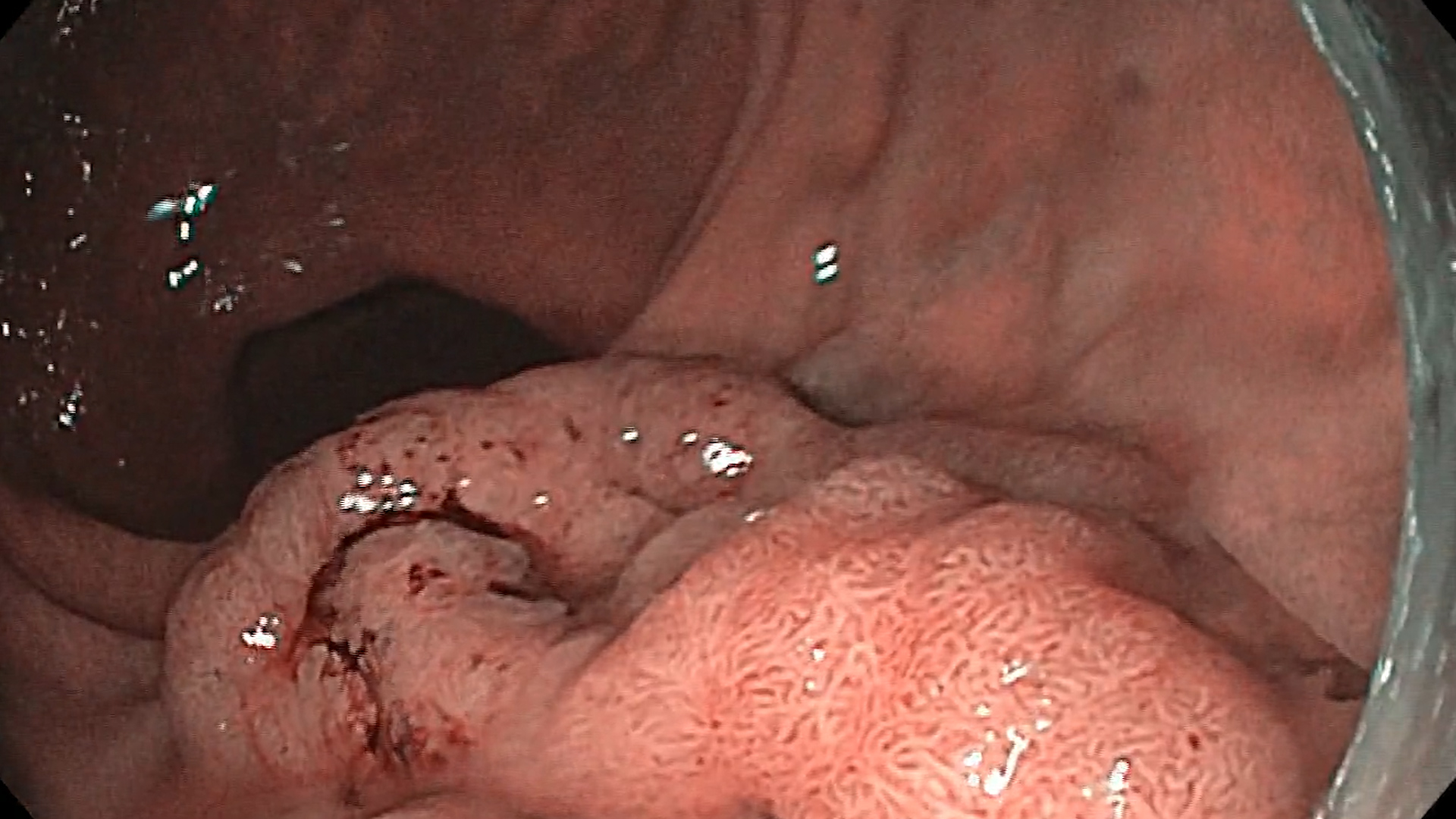
The technique of using a cold snare is different from resection with a hot snare. The lesion must be positioned at 5 o’clock, the tip of the catheter a few mm away and the snare must be fully open and placed completely over the lesion. Once placed completely over the polyp, the loop should be closed in a continuous maneuver (close and cut) while maintaining pressure on the snare and the colonic wall. When closed, the snare will also catch a margin of normal tissue. In the case of cold excision, the entrapped polyp should not be lifted during the maneuver in order to preserve the margin of normal tissue and keep the specimen in the loop. Often, after cutting, a central strip (ribbon) of submucous tissue can be visualized, which indicates the effectiveness of the polypectomy and the absence of damage to the submucosa, which is conglomerated in the central portion. After cutting, it can be irrigated with the jet wash pump, directly into the resulting submucosal defect: the elevation of the submucosa is obtained with the possibility of correctly examining the edges of the polypectomy and immediately controlling the resulting minimal bleeding. Immediate bleeding is usually insignificant and, usually, delayed bleeding does not occur.
An unsolved problem with the cold snare technique is how the endoscopist must handle the situation when the snare wire fails to cut the tissue and the snare remains captive in the wall, presumably because it captures too much submucosal tissue. Although this does not occur often, when dedicated cold polypectomy snares are used, it appears that lesions larger than 10 mm have the highest rate of incomplete resection. It is possible that repeated opening and/or closing maneuvers compromise the margin of normal tissue, resulting in histologically incomplete resection.
If the lesion fails to cut with the cold snare:
- Keep the snare tightly closed for 10-15 seconds
- Maintain full insufflation and avoid aspiration.
- Make sure the endoscope is straight.
- Angle the tip of the endoscope.
- Straighten and extend the catheter.
- Partially reopen the snare (about 1/3 of the snare handle; avoid fully opening). The goal is to open the snare wire just a little—enough to release the excess white ribbon of submucosa while keeping the snare “under” the lesion. It is important to avoid completely reopening the loop.
- Slowly lift the lesion off the colon wall.
- Be careful to release the trapped submucosa (a white band) under the lesion.
- Lower the lesion (to prevent its loss).
- Close the snare completely again to cut the lesion.
It is not known whether it is safe to apply electrocautery to a lesion that has failed to cut with the cold snare.
Diferențe între polipectomia la cald și la rece
| Cold snare | Hot snare | |
| The position of the lesion | At 5 o’clock | At 5 o’clock |
| Margins normal tissue | Yes : at least 2 mm | Partial : minimum |
| Angulation | No : the snare sheath must remain anchored to the colon wall | Da : for applying electrocautery |
| Closing the snare | Continue until the cut is complete | Temporarily stopping when resistance is felt |
| Aspiration | No : insufflation is maintained | Yes |
| Electrocautery | No | Yes |