See other cases
WOPN drainage and necrosectomy
History :
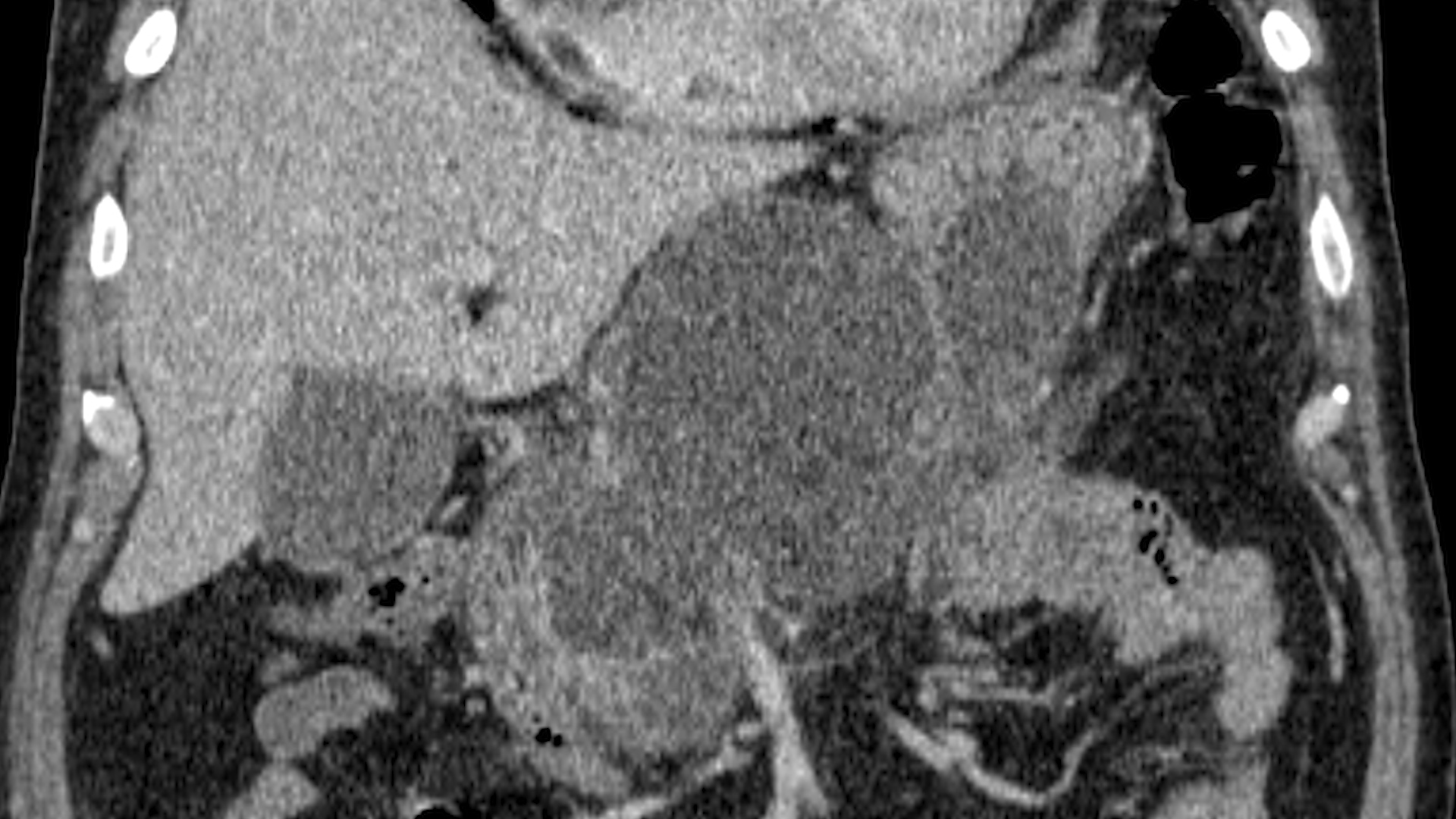
A 53-year-old man, smoker, with an episode of severe acute pancreatitis of uncertain etiology, complicated by a giant pancreatic collection, compressive at the gastric level, with necrosis inside (walled-off pancreatic necrosis) (Fig. 1-3).
Other conditions associated are represented by: arterial hypertension, psoriasis vulgaris and psoriatic arthritis for which he followed biological treatment with Guselkumab for 2 years.
Clinical & biological :
Clinical examination: psoriatic lesions on palms, abdomen slightly painful on deep palpation in the epigastrium.
Biological (at admission): inflammatory syndrome CRP =32 mg/L, FBG 565 mg/dL, without leukocytosis
MRI identified a peripancreatic collection of 12/6/7cm at the level of the pancreatic head, with necrotic material inside.
Imaging :
EUS Drainage:
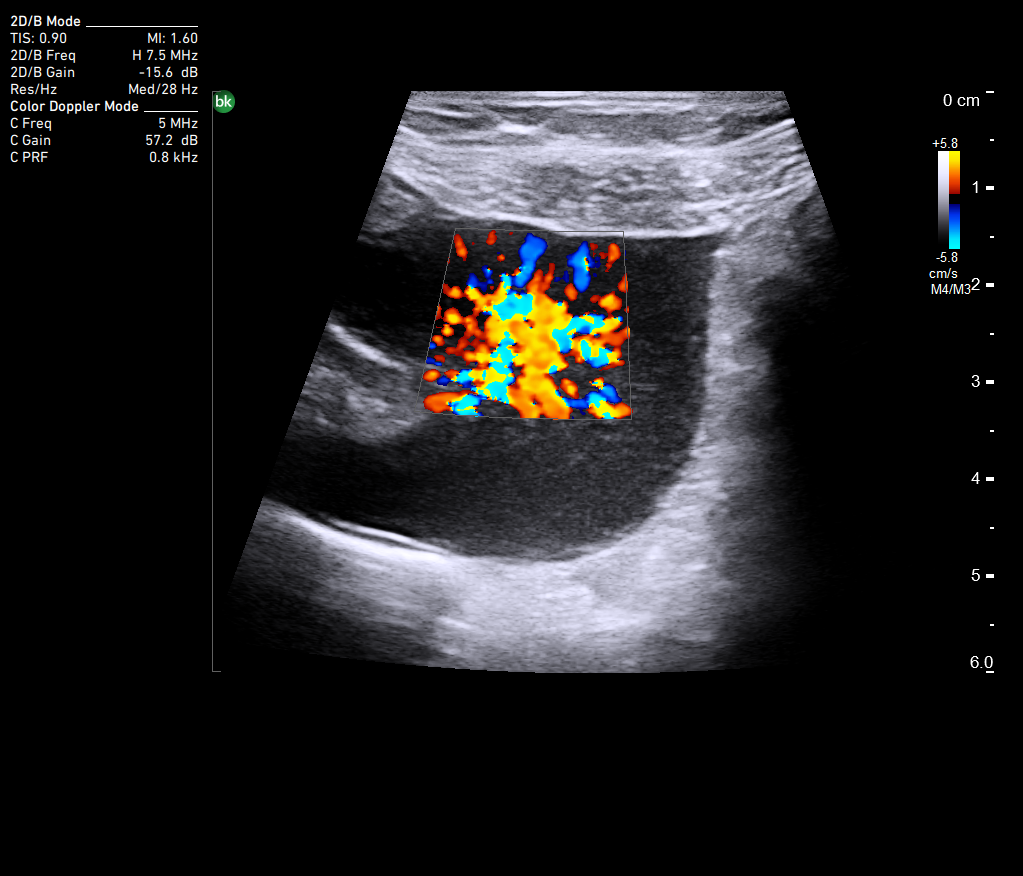
EUS examination highlights a peripancreatic collection with large dimensions (12/7/6 cm), with hyperechoic areas suggestive for necrosis (Movie 1). EUS-guided puncture was performed with a 19G needle and brown liquid was aspirated. Subsequently, a lumen apposing metal stent (LAMS) (HotAXIOS, Boston Scientific) of 15 mm was placed transgastrically, mounted on a 0.035 Fr guidewire, under EUS guidance and radiological guidance, with drainage of approximately 1000 mL of brown liquid (Fig. 3-4). Later, a double pigtail plastic stent was inserted through the LAMS stent (Fig. 5).
Post-procedural evolution; Necrosectomy:
Follow-up after one month showed a favorable evolution, with improved symptoms like pain, regression of the peripancreatic collection size and complete remission of the liquid component. However, there was a persistent inflammatory syndrome and fever was reported at home. Biologically the patient presented a high CRP of 25 mg/L, but negative blood cultures.
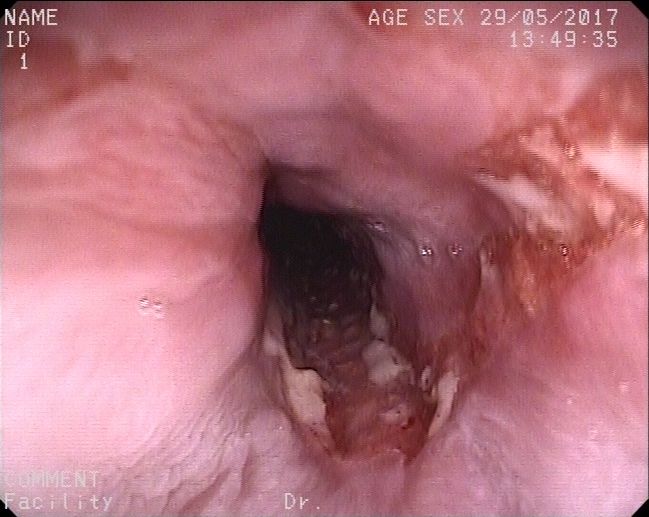
Direct endoscopic necrosectomy was performed (under general anesthesia with oro-tracheal intubation), with visualization at the level gastric body of the LAMS metal stent and the double pigtail plastic stent, both clogged with necrotic material. The double pigtail plastic stent was removed with a polypectomy loop. Dilation with a 15 mm CRE (controlled radial expansion) balloon of the LAMS was subsequently performed with visualization of the remaining cavity. Necrosectomy was performed with a polypectomy loop, identifying necrotic adhesions including viable pancreatic tissue that could not be extracted endoscopically (Fig. 6-7). Diffuse bleeding from the wall ensued and efficient endoscopic haemostasis was performed with a coagrasper. At the end of the procedure a 10 Fr double pigtail stent was placed through the metallic stent. The bacteriological examination of the necrotic material identified colonization with Pseudomonas aeruginosa and Klebsiella pneumoniae for which, with antibiotic therapy initiated according to the antibiogram.
Follow-up one week post-necrosctomy consisted of endoscopic re-evaluation with access of the remaining cavities. A large amount of remaining pancreatic necrosis was identifient, with an adherent nodule that was extracted with a polypectomy loop and Roth snare. The cavity was lavaged and the LAMS (HotAXIOS, Boston Scientific) was removed.
Diagnostic :
Infected walled-off pancreatic necrosis (WOPN) after acute pancreatitis of uncertain etiology > endoscopic ultrasound (EUS) drainage with LAMS and gradual direct endoscopic necrosectomy.
Discussion :
Walled-off pancreatic necrosis (WON) is a late stage complication of acute pancreatitis, leading in some cases to symptoms such as abdominal pain, signs and symptoms of gastrointestinal obstruction by extrinsic compression or bacterial superinfection. Transgastric drainage guided by EUS consisting of LAMS type transluminal expandable metallic stent is a first-line option regarding risk / benefit ratio, as compared to the percutaneous or surgical approaches. Direct endoscopic necrosectomy represents a “more” aggressive approach of “step-up” treatment by extracting direct necrotic content from the WOPN cavity.
Conclusion :
Endoscopic ultrasound (EUS) drainage of the peripancreatic necrotic collections (WOPN) is a minimally invasive alternative to surgical treatment or percutaneous drainage because of efficient and quick results, being associated with a lower rate of morbidity and mortality.
References :
- Mukai S, Sofuni A, Tsuchiya T, Tanaka R, Tonozuka R, Matsunami Y, Nagai K, Kojima H, Minami H, Hirakawa N, Asano K, Shionoya K, Hama K, Itoi T. Endoscopic Step-up Approach for Walled-off Necrosis After Acute Pancreatitis. DEN Open. 2025 Aug 25;6(1):e70188. doi: 10.1002/deo2.70188. PMID: 40860854; PMCID: PMC12375900.
- Nemoto Y, Attam R, Arain MA, Trikudanathan G, Mallery S, Beilman GJ, Freeman ML. Interventions for walled off necrosis using an algorithm based endoscopic step-up approach: Outcomes in a large cohort of patients. Pancreatology. 2017 Sep-Oct;17(5):663-668. doi: 10.1016/j.pan.2017.07.195. Epub 2017 Jul 31. PMID: 28803859.
- Pattarapuntakul T, Charoenrit T, Wong T, Netinatsunton N, Ovartlarnporn B, Yaowmaneerat T, Tubtawee T, Boonsri P, Sripongpun P. Clinical Outcomes of the Endoscopic Step-Up Approach with or without Radiology-Guided Percutaneous Drainage for Symptomatic Walled-Off Pancreatic Necrosis. Medicina (Kaunas). 2023 Mar 14;59(3):569. doi: 10.3390/medicina59030569. PMID: 36984570; PMCID: PMC10058734.
- Yuen R, Lam B, Chan SM, Yip HC, Teoh AYB. Comparison of Direct Endoscopic Necrosectomy With Endoscopic Step-Up Approach After Endoscopic Drainage of Pancreatic Walled-Off Necrosis: Systematic Review and Meta-Analysis. Dig Endosc. 2025 Dec;37(12):1286-1294. doi: 10.1111/den.70021. Epub 2025 Sep 2. PMID: 40898808.