See other cases
Endoscopic resection of a complex colonic polyp
History :
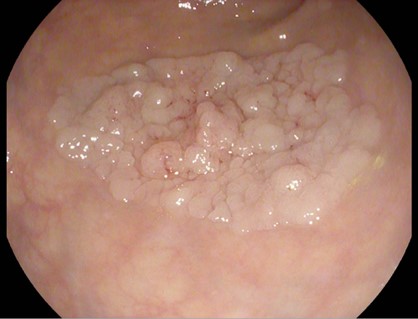
A 49-year-old male patient, who performed a previous colonoscopy that showed a pedunculated polyp of 40 mm in diameter situated on the descending colon, with high grade dysplasia on histology, is admitted in our clinic to perform a polypectomy.
Clinical & biological :
The blood tests showed normal levels of CA19-9, CEA, PSA, without an inflammatory syndrome, without anemia and normal coagulation markers.
Imaging :
The CT scan he did in November 2023 showed no metastases and no suspicious parietal thickenings at the level of the scanned digestive tube segments.
Diagnostic :
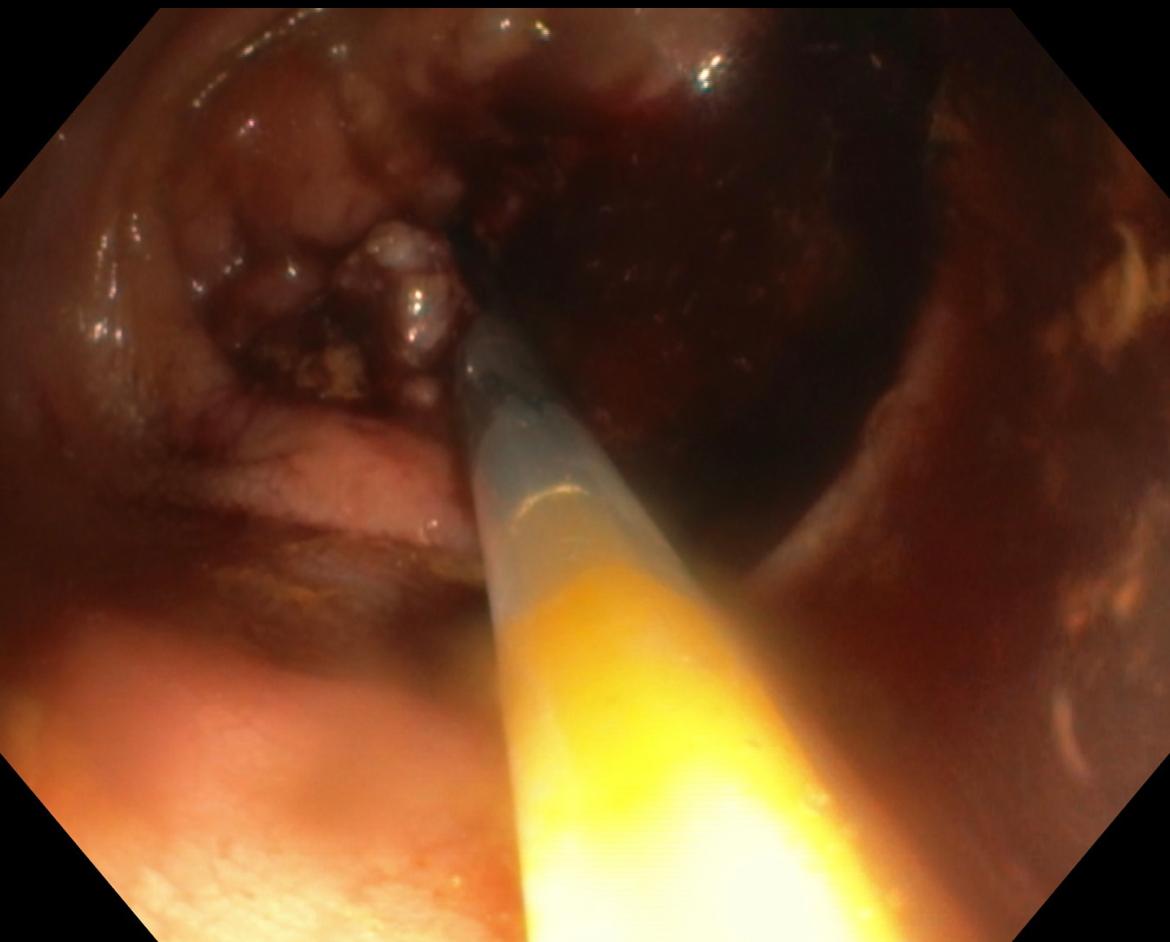
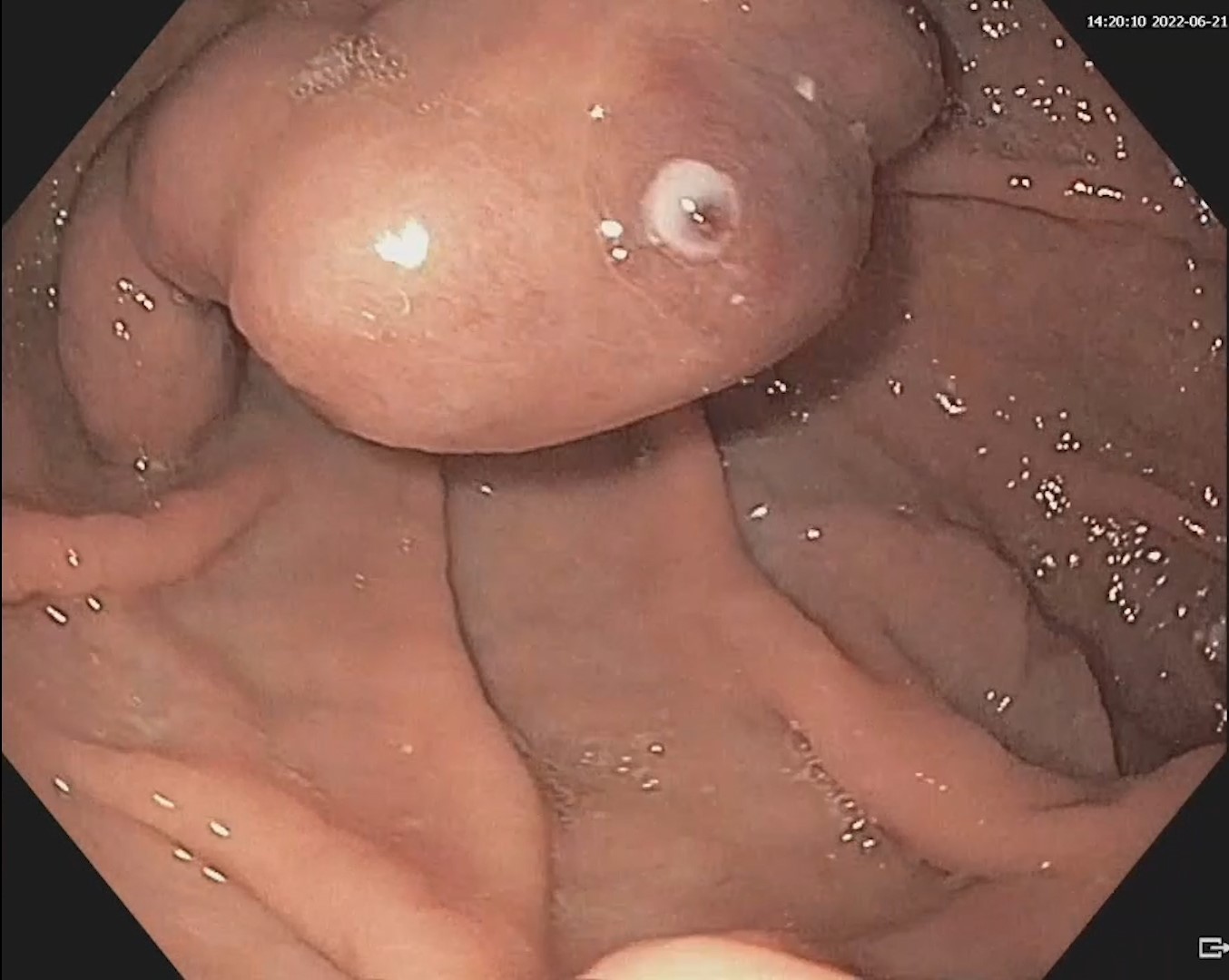
The colonic polyp was classified as Paris Ip, NICE II, JNET 2B, SMSA 4. To perform resection, an endo-loop was placed at the base of the pedicle and the polyp was resected above the endo-loop using a 30 mm hot snare. 3 hemo-clips of 20 mm were placed at the base of the polyp after resection with no obvious bleeding at the end of the procedure.
The histological examination showed a well differentiated adenocarcinoma (G1), developed on the background of a tubule-villous adenoma with high grade dysplasia, pT1 (invasion through the muscularis mucosa but limited to the submucosa), Nx, Mx, L0 V0(absence of lympho-vascular and venous invasion), R0 (microscopically margin-negative resection – with a resection margin situated at 8mm of the tumor), Haggit 2 (tumor cells invading the level of the neck of the polyp), TB1 (low budding with 0-4 buds observed in the front of the invasion).
Discussion :
There are multiple methods to perform a polypectomy (cold snare, hot snare, injection with either saline or epinephrine, clip assisted, endo-loop assisted, EMR, ESD).
United States Multi-Society Task Force [1] recommends mechanical ligation (pre-resection) for the polyps that have a head size above 20 mm and a stalk thickness more than 5 mm. Ligation is done either with clips or endo-loops with the aim of reducing blood flow to the head of the polyp, subsequently shrinkage making it easier to maneuver snares around the head of the polyp. Additionally, it reduces the rate of post-polypectomy bleeding. Complete resection according to histological examination (Haggitt 2, well differentiation, L0, V0, more than 1 mm resection margins) requires a surveillance colonoscopy in 1 year [2, 3].
Conclusion :
This case highlights the significance of regular screening and surveillance colonoscopy in early detection and prevention of colorectal cancer. The complete resection with clear margins is essential for preventing recurrence and reducing the risk of cancer progression.
References :
- Kaltenbach T, Anderson JC, Burke CA, Dominitz JA, Gupta S, Lieberman D, Robertson DJ, Shaukat A, Syngal S, Rex DK. Endoscopic Removal of Colorectal Lesions-Recommendations by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2020; 91(3): 486-519.
- Symer M, Connolly J, Yeo H. Management of the malignant colorectal polyp. Curr Probl Surg 2022; 59(5): 101124.
- Hassan C, Wysocki PT, Fuccio L, Seufferlein T, Dinis-Ribeiro M, Brandão C, Regula J, Frazzoni L, Pellise M, Alfieri S, Dekker E, Jover R, Rosati G, Senore C, Spada C, Gralnek I, Dumonceau JM, van Hooft JE, van Cutsem E, Ponchon T. Endoscopic surveillance after surgical or endoscopic resection for colorectal cancer: European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Digestive Oncology (ESDO) Guideline. Endoscopy. 2019; 51(3): C1.