See other cases
A rare cause of malabsorption syndrome
History :
A 67-year-old patient with chronic diarrhea for more than 1 year, with negative serological tests for celiac disease, Clostridium difficile toxin and cultures, but with persistent iron deficiency anemia and marked weight loss (25 kg in the last 6 months).
Clinical & biological :
Clinical: pallor, dehydration signs.
Paraclinical: iron deficiency anemia (hemoglobin = 9.5 g/dL, serum iron = 20 mg/dL), severe hypoalbuminemia (albumine = 1.5 g/dL), increased serum creatinine and blood urea nitrogen.
Imaging :
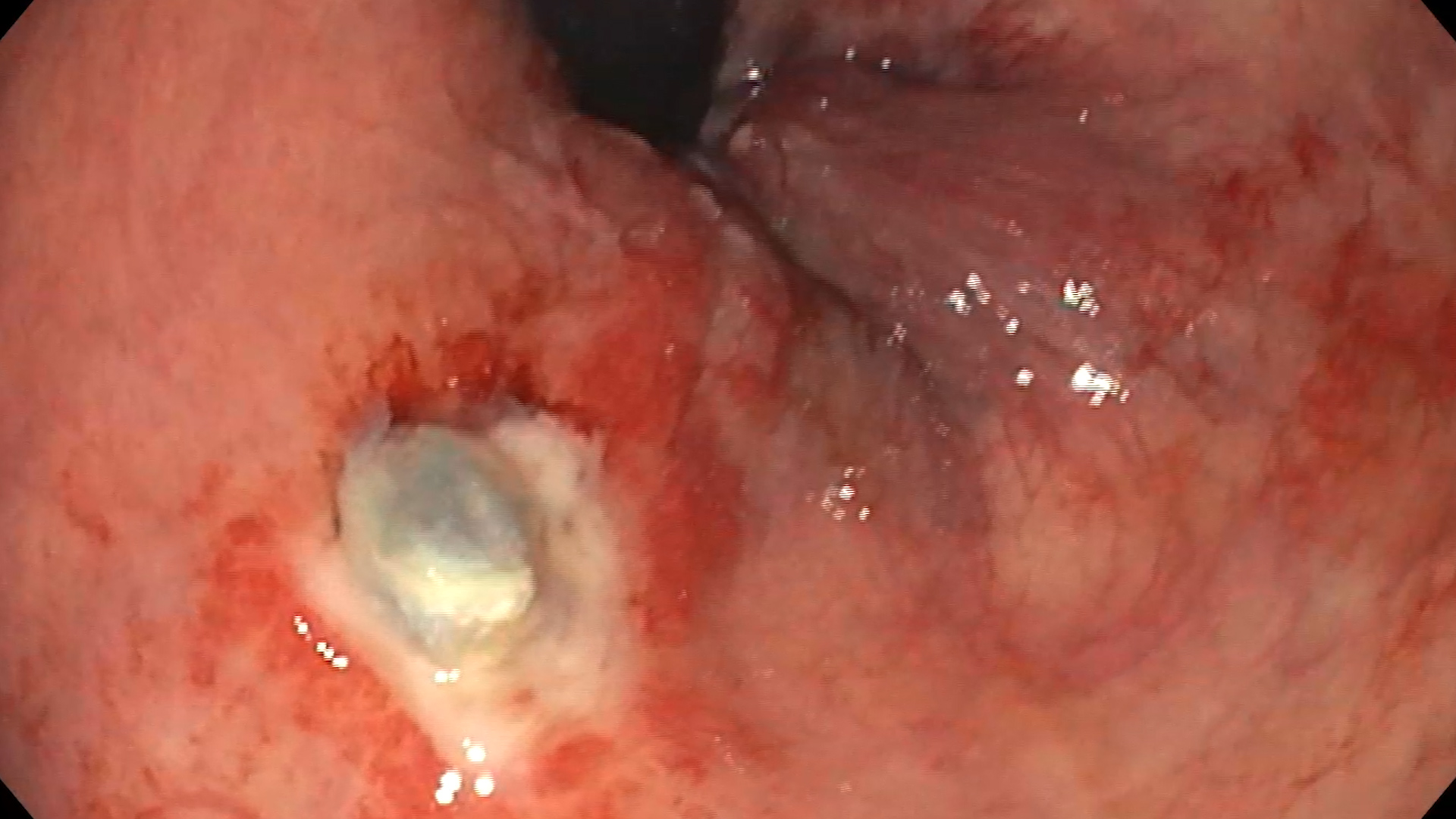
Video capsule endoscopy revealed diffuse erythema, edema and multiple scattered whitish plaques (Figure 1 and Figure 2, Video 1).
Diagnostic :
Duodenal and terminal ileum biopsies revealed diffuse infiltration with positive macrophages in PAS staining, suggestive of Whipple’s disease.
Discussion :
Whipple disease is a rare condition caused by a gram-positive bacterium, Tropheryma whipplei. The disease is a systemic infection that mainly affects the small intestine, but can also develop as seronegative arthritis or infectious endocarditis. The clinical picture is extremely polymorphic, with nonspecific symptoms that can easily simulate other conditions. The definite diagnosis includes histopathological examination with PAS positive macrophages and/or PCR examination targeting the 16S rRNA gene of Tropheryema whipplei on small bowel biopsies. The treatment is based on Ceftriaxone for 2 weeks (2 g/day) or Meropenem (1g/day) for 2 weeks (in the forms with neurological impairment in which the penetration of the blood-brain barrier is necessary), followed by maintenance treatment with Trimethoprim-Sulfamethoxazole (160/800 mg x 2/day) for at least 1 year. Alternatively, Doxycycline (200 mg/day) in combination with Hydroxychloroquine (600 mg/day) may be used for 1 year. Due to the risk of recurrence, annual endoscopic follow-up is usually required.
Conclusion :
Although rare, Whipple’s disease should be part of the evaluation of chronic diarrhea, and video capsule endoscopy may indicate changes suggestive for the diagnosis of this disease.
References :
1. Tison A, Preuss P, Leleu C, Robin F, Le Pluart A, Vix J, Le Mélédo G, Goupille P, Gervais E, Cormier G, Albert JD, Perdriger A, Bouvard B, Berthelot JM, Foulquier N, Saraux A; network of rheumatologists from the Grand Ouest “VICTOR HUGO”. Rheumatological features of Whipple disease. Sci Rep 2021; 11(1): 12278.
2. Melas N, Amin R, Gyllemark P, Younes AH, Almer S. Whipple’s disease: the great masquerader-a high level of suspicion is the key to diagnosis. BMC Gastroenterol 2021; 21(1): 128.
3. Lagier JC, Raoult D. Whipple’s disease and Tropheryma whipplei infections: when to suspect them and how to diagnose and treat them. Curr Opin Infect Dis 2018; 31(6): 463-470.
4. De Francesco V, Corsi F, Pennella A, Bellesia A, Fiorini G, Vaira D, Zullo A. Whipple’s disease: case report and review of the literature. J Gastrointestin Liver Dis 2018; 27(3): 331-336. 5. Biagi F, Biagi GL, Corazza GR. What is the best therapy for Whipple’s disease? Our point of view. Scand J Gastroenterol 2017; 52(4): 465-466.