See other “How to”
The alphabet soup of polyp optical diagnosis
Description :
Colorectal Cancer (CRC)
> a significant public health issue
> the 2nd leading cause of cancer-related mortality worldwide
> 70%-90% have adenomatous polyps as precursors (prevention through screening colonoscopy)
Classification of Polyps
> Currently, there are 3 main categories defined
- hyperplastic polyps (benign)
- adenomatous polyps (premalignant)
- sessile serrated polyps account for approximately 15-30% of colorectal cancer cases (Figure 1)
> Size is essential > ~ 90% of resected polyps are < 10 mm, with 70-80% being diminutive (<5 mm)
- only ~ 0.5% of diminutive polyps (< 5mm), and 1.5% of small ones (6-9 mm), are histologically advanced
- important strategies
- “resect & discard” versus “diagnose & leave-in”
- increasing withdrawal time (6 min > 9 min)
- virtual chromoendoscopy (sequential red-green-blue illumination, modifying the conventional white light source with special filters (NBI-Narrow Band Imaging) or special software (FICE; I-scan)
- NICE (NBI International Colorectal Endoscopic) or J-NET (Japan NBI Expert Team) classification
> NICE classification, based on color, vessel appearance, and polyp surface
- good accuracy for differentiating between hyperplastic (type 1) and adenomatous (type 2) polyps
- low accuracy in identifying sessile serrated polyps, often considered hyperplastic polyps
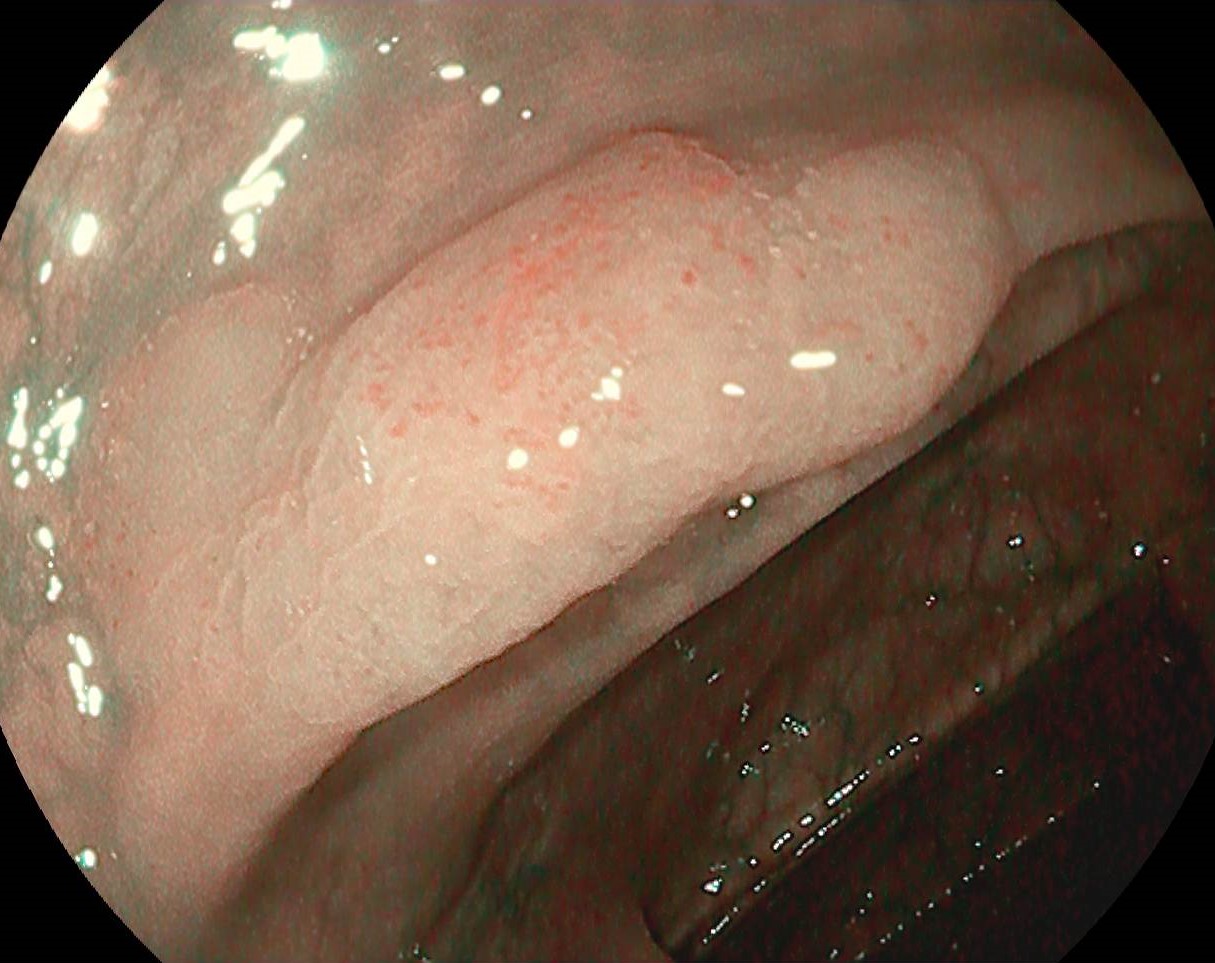
> WASP classification introduced in 2016 by the Workgroup Serrated Polyps and Polyposis (WASP)
- combines the NICE classification and criteria proposed by Hazewinkel et al.
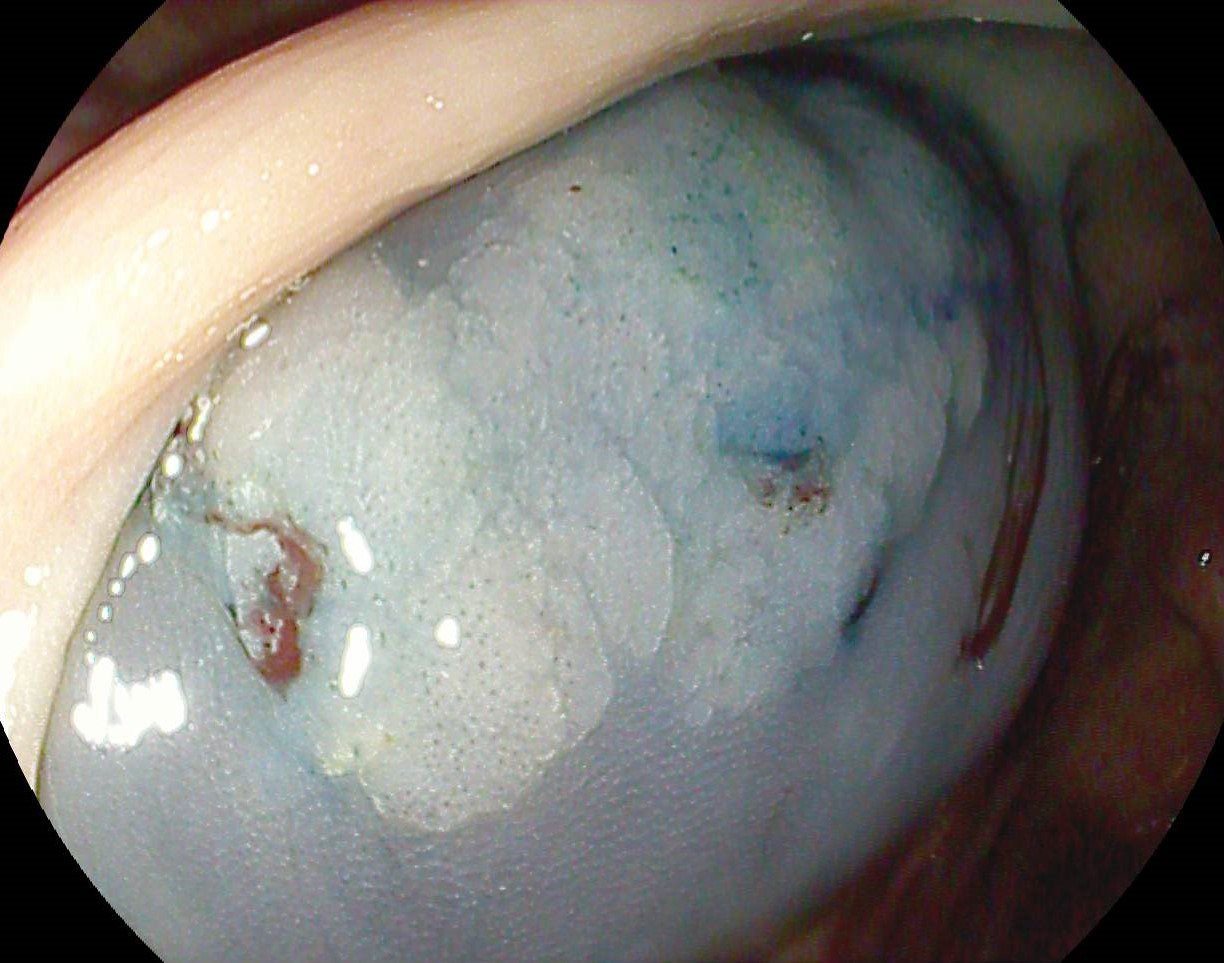
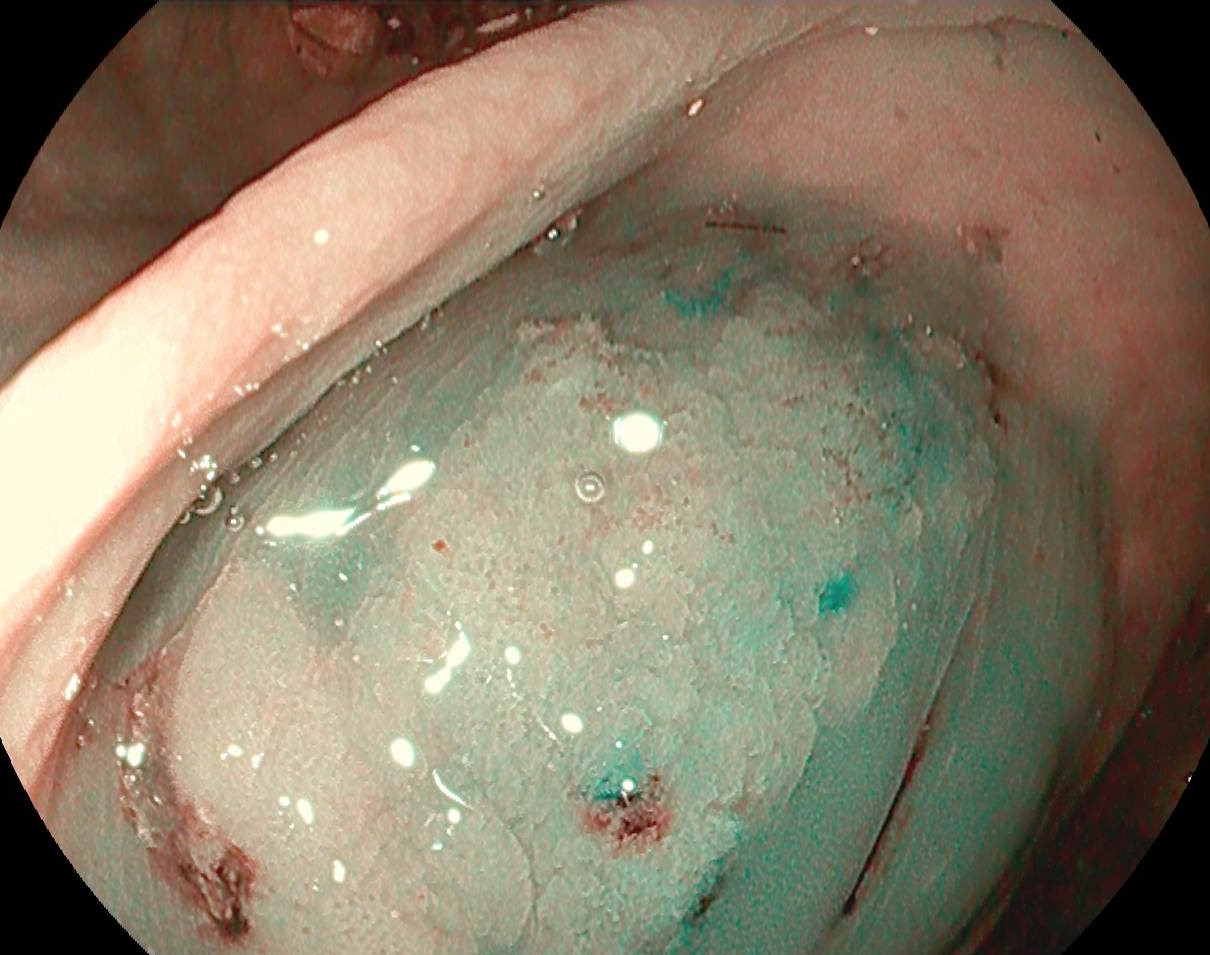
- irregular surface – cloud-like appearance
- indistinct borders
- irregular shape
- dark spots inside the crypts
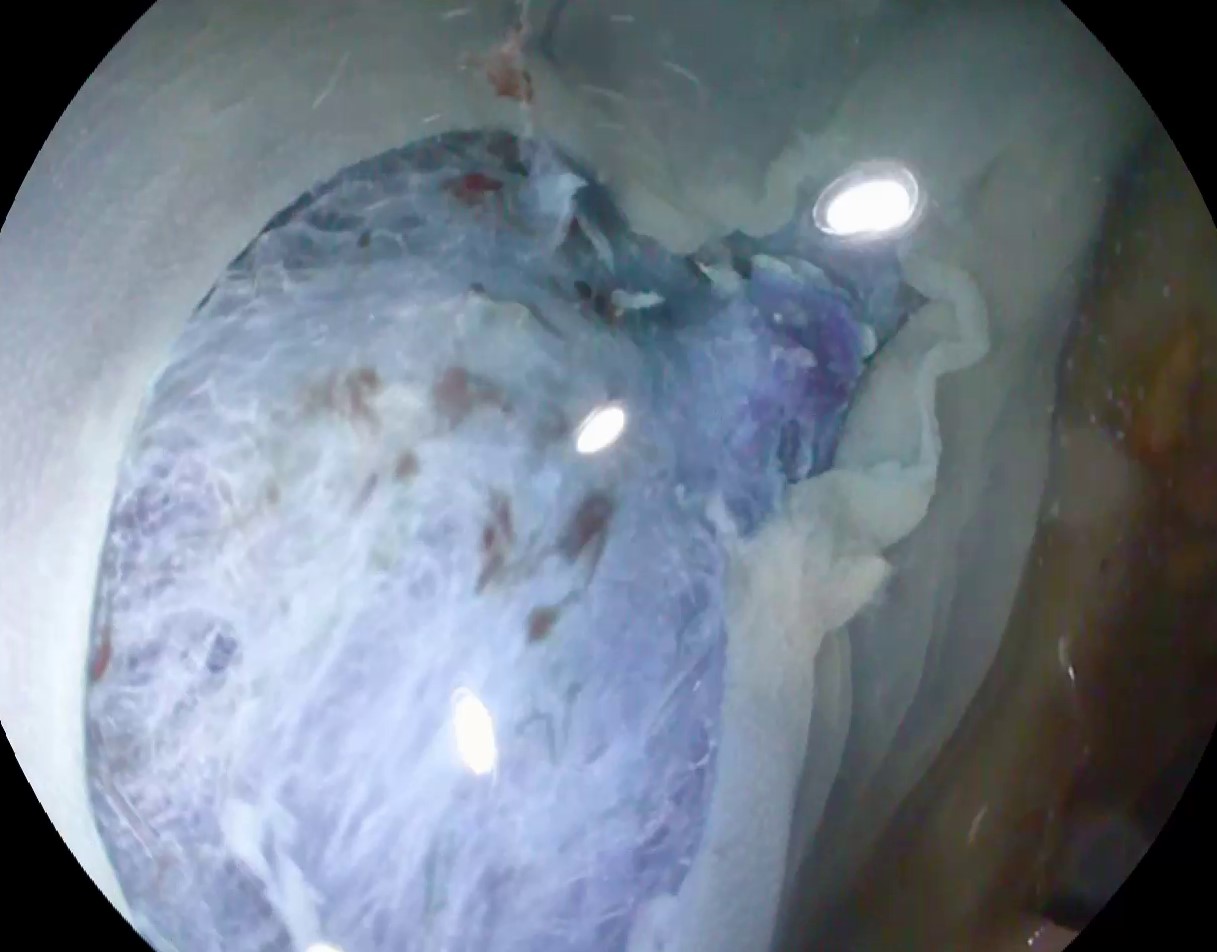
- the objective of the WASP classification
- to differentially diagnose between hyperplastic, conventional adenomatous, and sessile serrated polyps < 10 mm, in a step-wise evaluation (Figure 2)
- Step 1 – applying the NICE classification criteria and categorizing into one of the 2 nonspecific sessile serrated polyps (NICE 1 versus NICE 2)
- Step 2 – applying specific criteria for sessile serrated polyps – the presence of at least 2 of these criteria is sufficient for diagnosis
- to differentially diagnose between hyperplastic, conventional adenomatous, and sessile serrated polyps < 10 mm, in a step-wise evaluation (Figure 2)
> Good to know
- modified SANO classification
- includes sessile serrated polyps (SSP) / sessile serrated adenomas (SSA) – MS type Iio
- recent comparative studies have shown the superiority of the MS score in identifying SSA/SSP compared to WASP+NICE and WASP+J-NET, respectively
- confocal laser endomicroscopy (CLE) > allows “optical biopsy,” possibly playing a role in diagnosing SSP/SSA
-
serrated polyposis syndrome > 3-5 times higher risk of developing CRC compared to the general population > follow-up colonoscopy every 3 years (according to ESGE recommendations)