See other “How to”
Hemostasis by injection
Description :
Endoscopic hemostasis is essential both for the management of acute GI bleeding and for performing advanced interventional procedures such as endoscopic submucosal dissection (ESD), where hemostasis is considered part of endoscopic therapy and not an adverse event.
Usually, for endoscopic hemostasis, 3-4 standard techniques are used :
- I.injection therapy
- II.mechanical hemostasis (clips, endo-loop, ligatures)
- III.thermo-coagulation (tweezers, mono or bipolar probes)
- IV.argon plasma coagulation
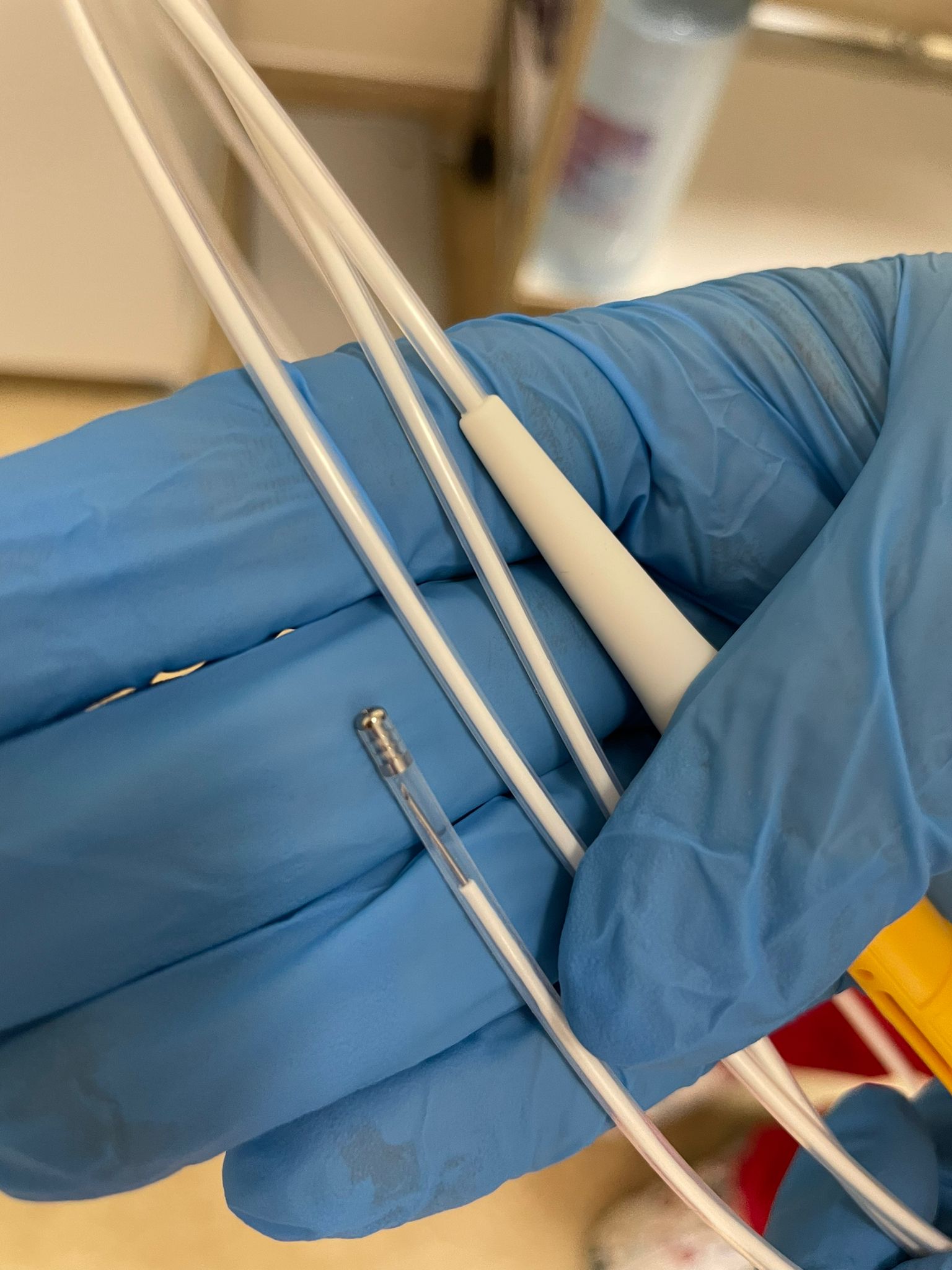
I.1. Injection needle
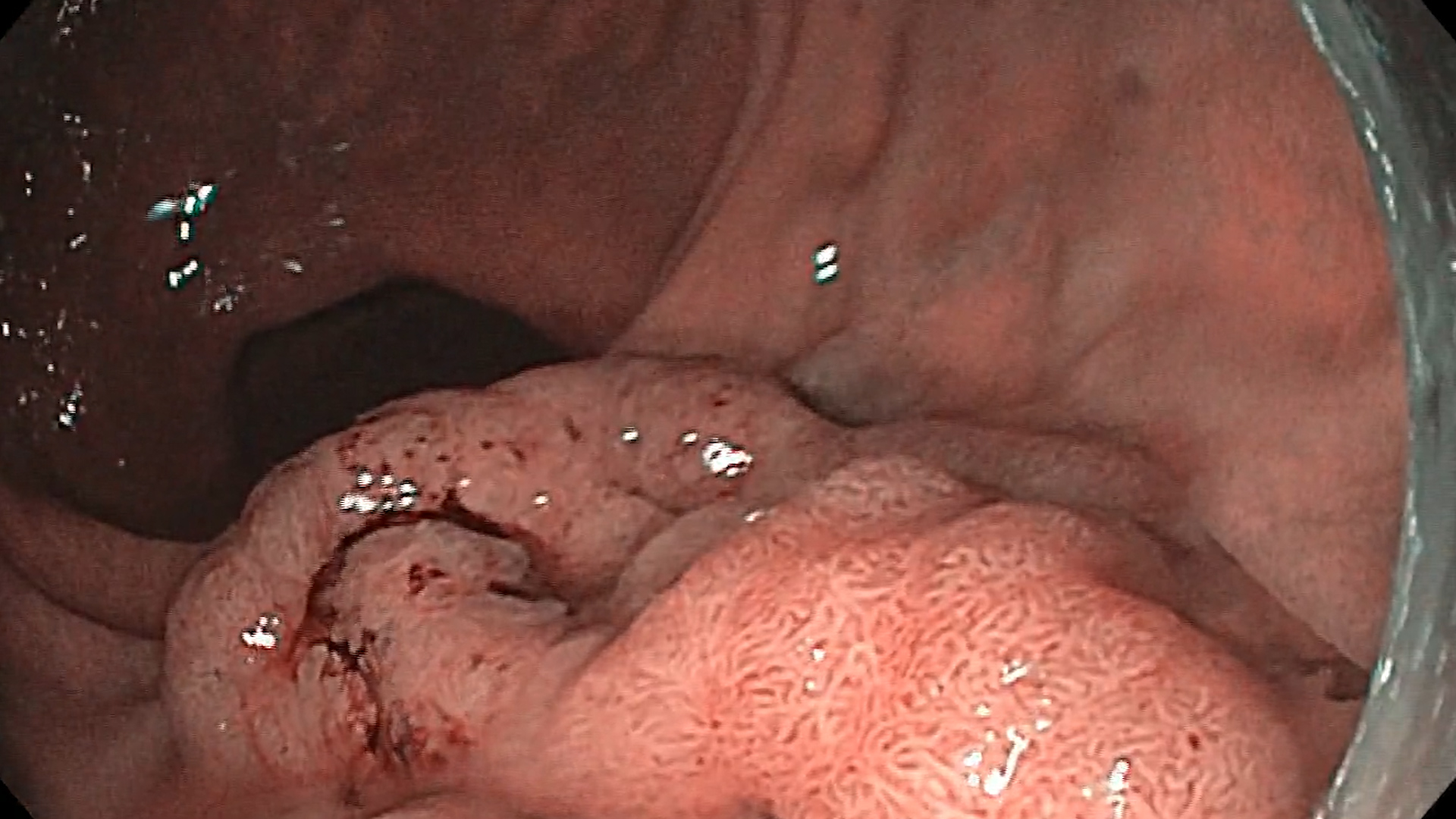
Injection therapy is the oldest technique and usually involves the injection of adrenaline. Diluted adrenaline (1:10 000) is available worldwide, and probably the simplest treatment for bleeding. Usually 10 to 40 ml is injected. If used alone, there is a significant risk of rebleeding which can be reduced by injecting larger volumes. But, pay attention to the risk of adverse cardiovascular events.
The injection needle is single use, with a longer size for colonoscopy and a shorter one for upper endoscopies. Before use, its exterior is checked, the syringe is attached, the agent is inserted into the catheter, it works on the push and pull principle. We remove the needle, inject, withdraw the needle. And we take it out, inject it, withdraw it.
The needle is easy to use, even in tangential lesions when the tip of the endoscope is angled. It is injected according to the doctor’s instructions, 2 ml each. The nurse must be careful to withdraw it into its plastic sheath before the physician fully withdraws the catheter into the working channel.
Other agents, such as sclerosing agents, polidocanol, have similar efficacy but with more side effects.