See other “How to”
Endoscopic polypectomy
Description :
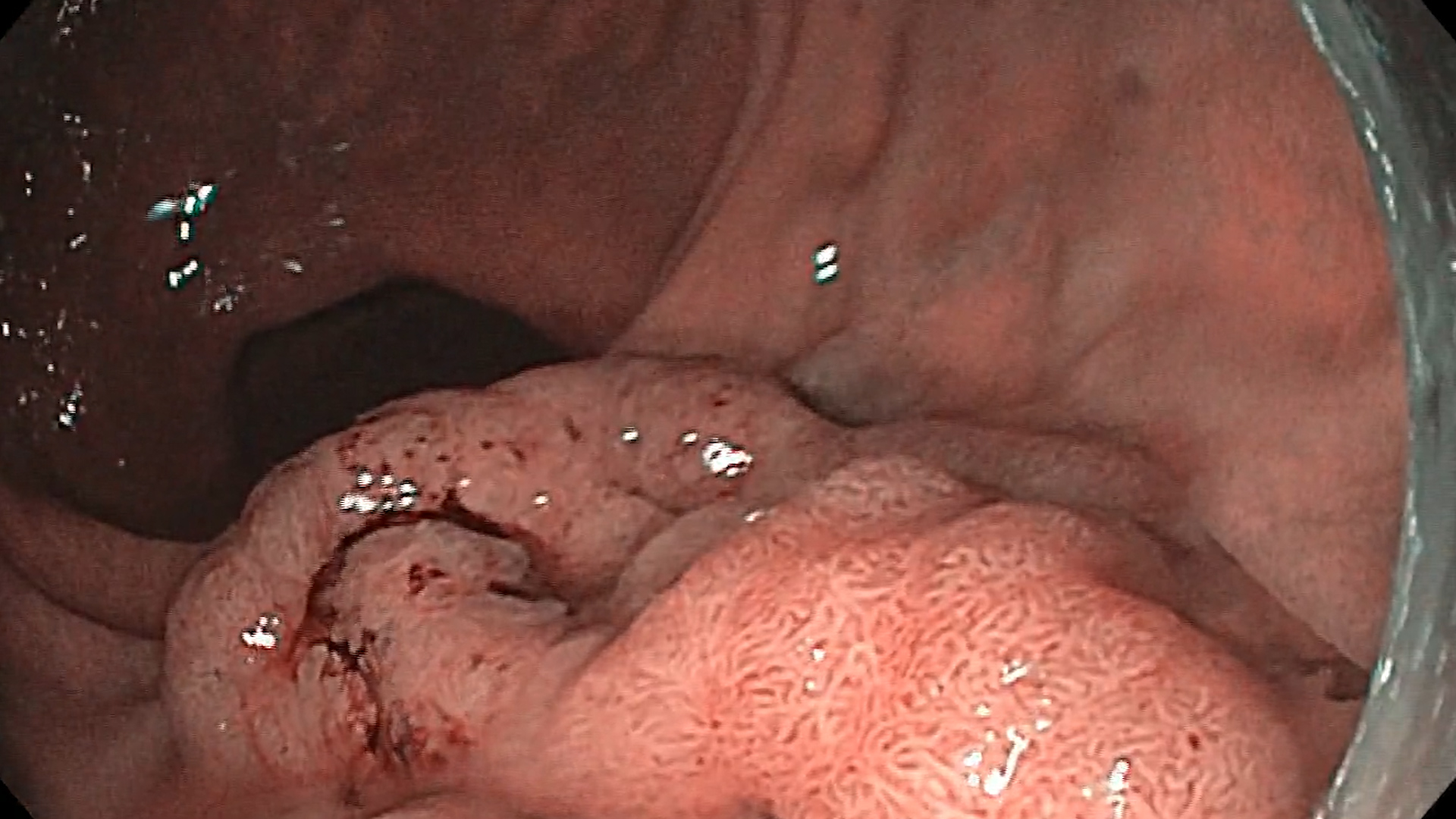
Polypectomy is the most common and arguably the most important procedure in digestive endoscopy. The main goal of polypectomy is the complete removal of the polyp and the subsequent prevention of colorectal cancer:l: Polypectomy examples
Before the procedure:
– Make sure that everything is already prepared and that it is in the examination room including the medication and devices for hemostasis. Make sure everything is working (electrocautery, wash pump, CO2 insufflation, etc).
– Monitor the patient throughout the procedure.
– Hygiene is an essential issue for both the patient and the staff. Wash your hands often, wear gloves, mask and glasses, protective equipment.
– Good cooperation between doctor and nurse contributes to the success of the procedure.
During the procedure:
– The choice of a correct loop is essential for the procedure: the snare used for hot polypectomy has thick and braided wire, various sizes (10-35 mm) and shapes (oval, asymmetrical, hexagonal).
– The major factor in the occurrence of post-polypectomy adverse events (bleeding, perforation, post-polypectomy syndrome, etc.) is electrocauterization.
– The method of polypectomy is chosen according to the size of the polyp.
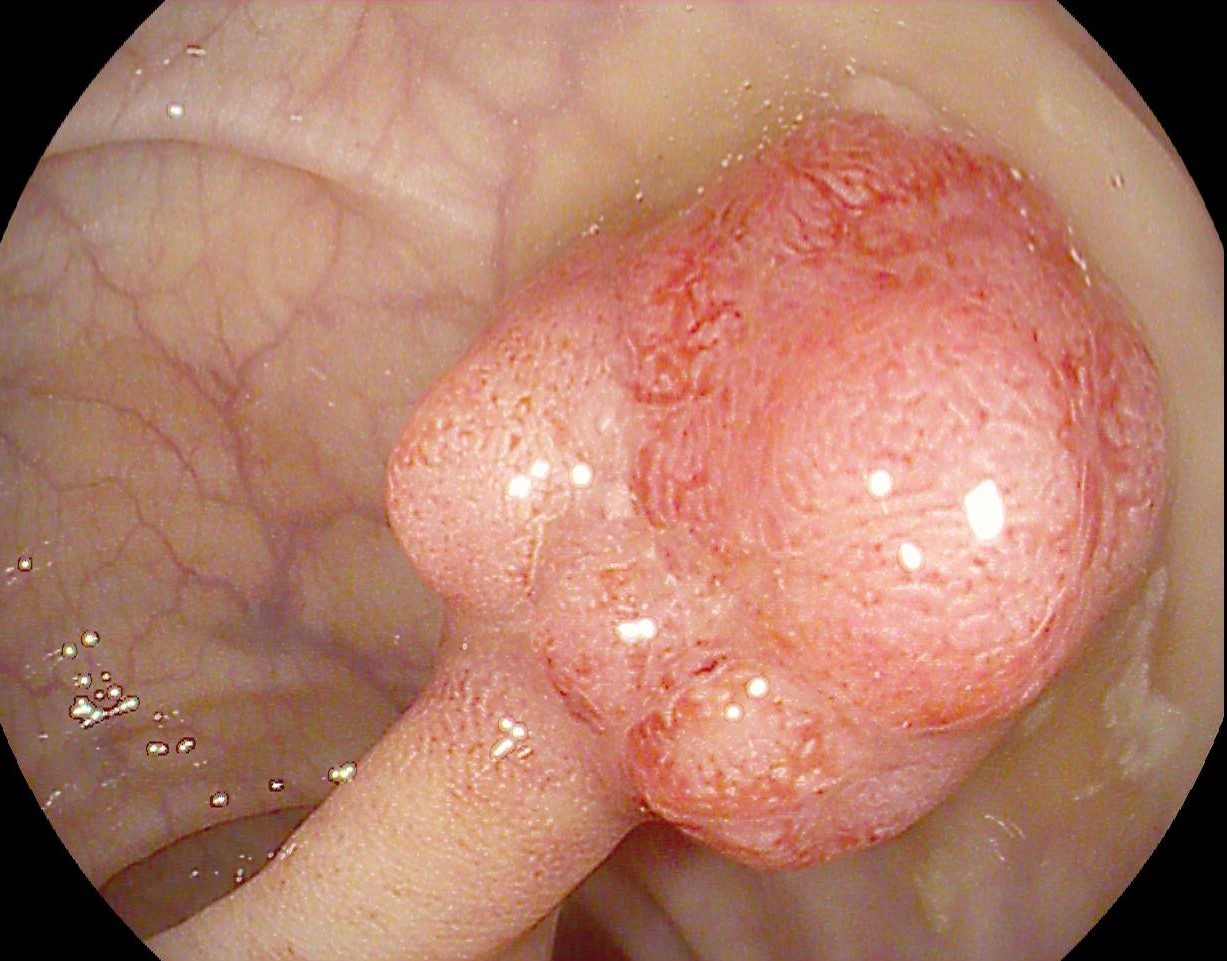
- Pediculated polyps
1a. Pedicled polyps with a thin pedicle (< 5 mm) or small polyp head (< 20 mm) can be directly resected with hot snare polypectomy by placing the snare midway through the pedicle (Movie 1).
1b. For polyps with a thick pedicle (> 5 mm) or a large polyp head (> 20 mm)it is recommended to use the endo-loop (Movie 2) or place metal clips (Movie 3) at the base of the pedicle, for bleeding prophylaxis. After that, a polypectomy loop and coagulation + cutting (blended) current can be used.
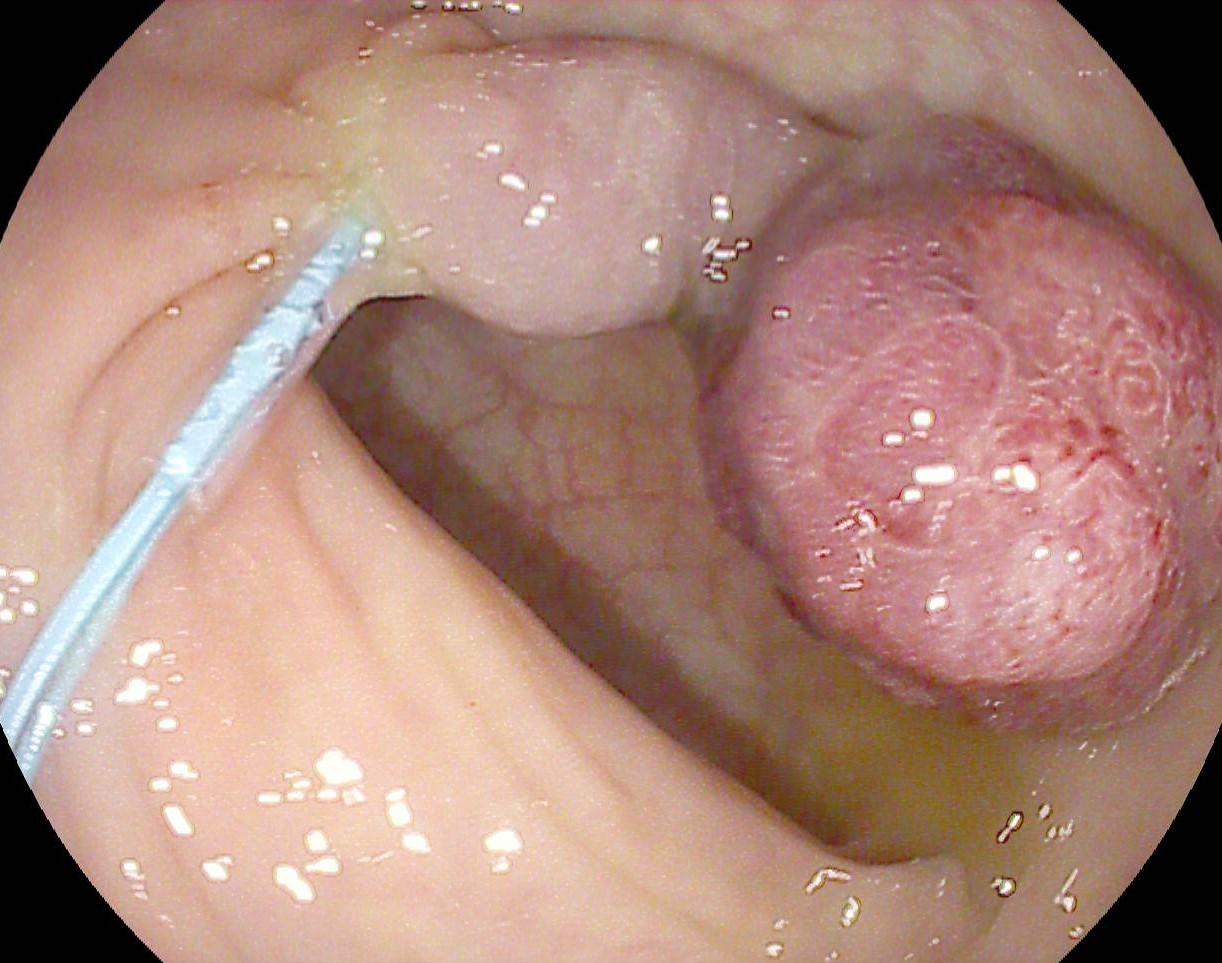
- Sessile / flat polyps
2a. Small polyps (< 10 mm) are generally resected by cold snare polypectomy – CSP (Movie 4).
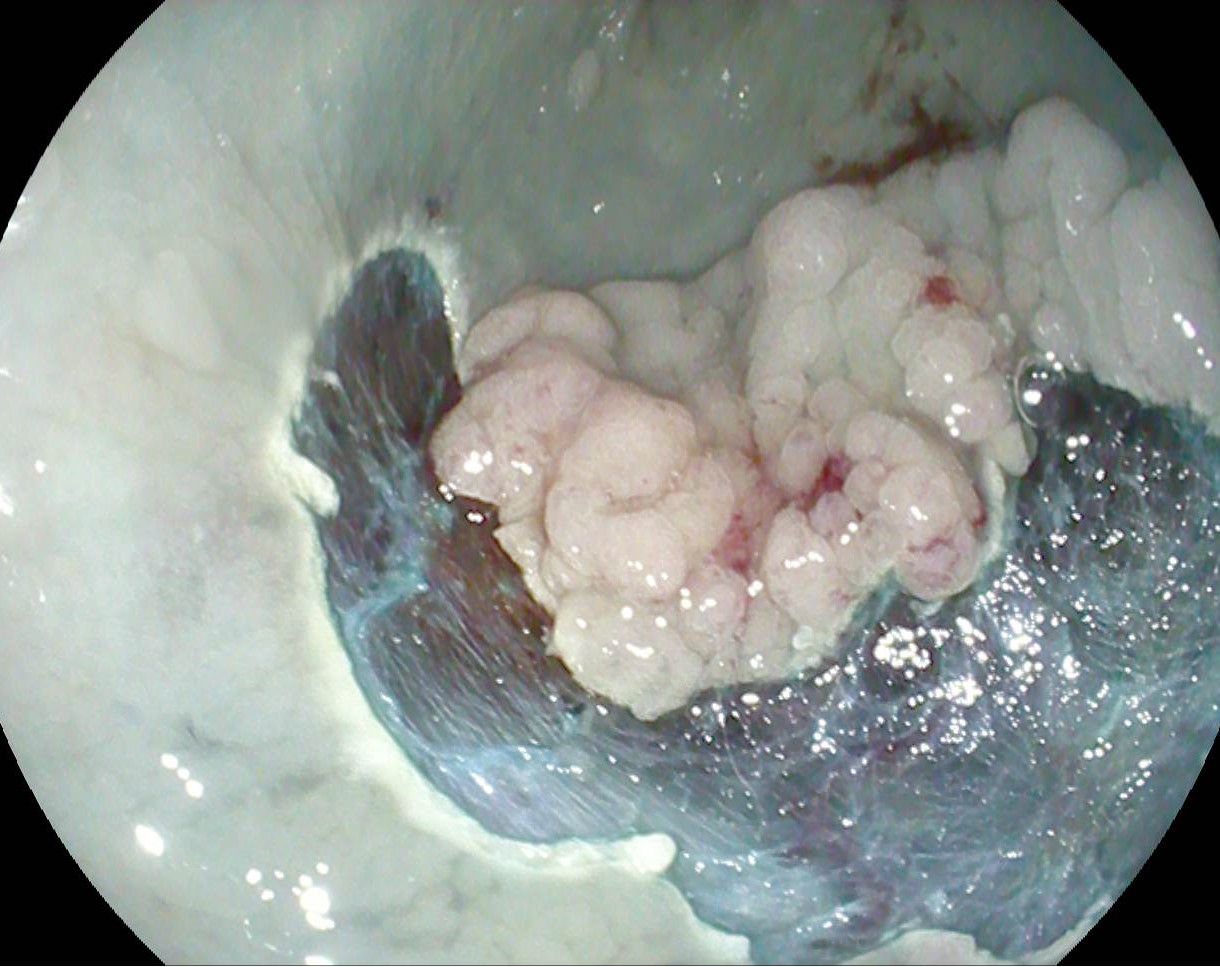
2b. For sessile / flat polyps of 10-20 mm, hot snare polypectomy is generally indicated, after submucosal injection (usually inject the submucosa with adrenaline 1:10 000 dissolved in saline or preferably Gelofusine, with a few drops of methylene blue). Injection of methylene blue is useful for coloring the submucosa and identifying possible complications, with muscle damage (target sign/perforation), which requires closing the resulting defect with clips. En bloc resection of flat polyps is recommended so that the resection margins can be properly evaluated (Movie 5).
2c. For sessile / flat polyps over 20 mm endoscopic mucosal resection (EMR) is used. This is generally done by injection, to elevate the lesion from the muscle layer and create a safety zone. Loops with thin, flexible wire are used, crescent-shaped ones are rarely recommended (Movie 6).