See other “How to”
Contrast-enhanced ultrasound > HCC vs CCC
Description :
In the evaluation of the liver using contrast-enhanced ultrasound (CEUS), the follow-up of the portal venous and late phases brings a significant contribution to the differential diagnosis of liver focal lesions: both between benign and malignant ones, as well as within malignant ones. A rapid onset and an increased intensity of the wash-out phenomenon are often associated with cholangiocarcinomas (iCCC), respectively liver metastases, while hepatocarcinoma (HCC) shows a late wash-out (often after 2-3 minutes), being of a lower intensity.
Typical CEUS aspects for
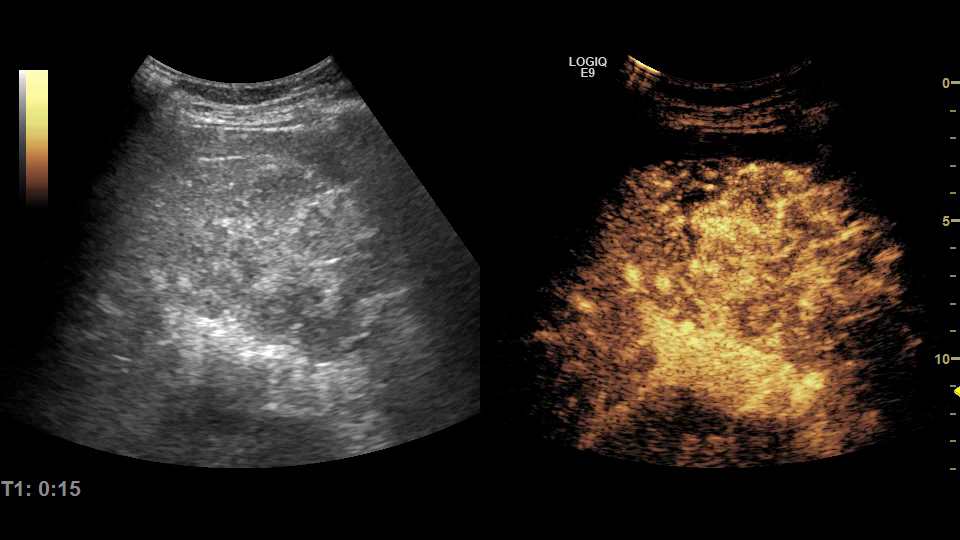
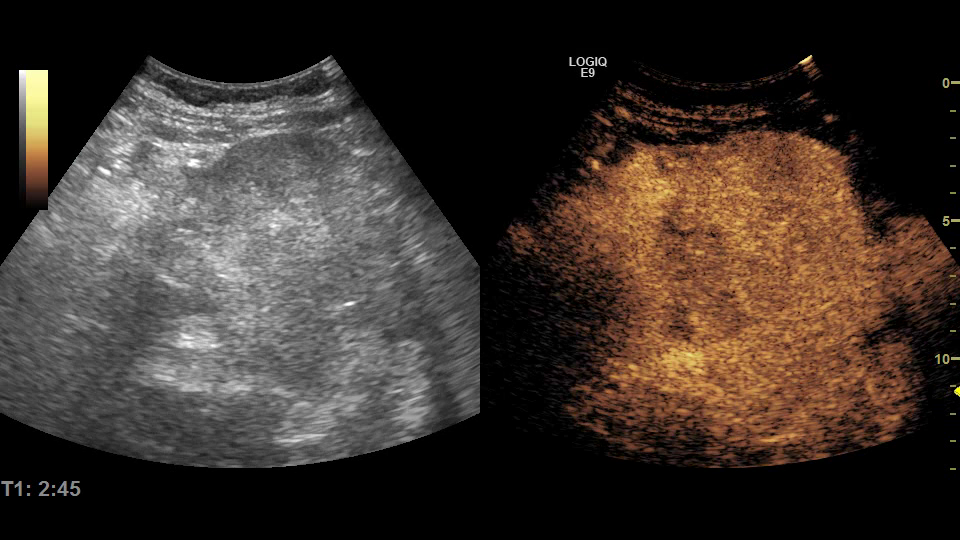
> HCC (Fig. 1 – arterial hyperenhancement & Fig. 2 – late wash-out)
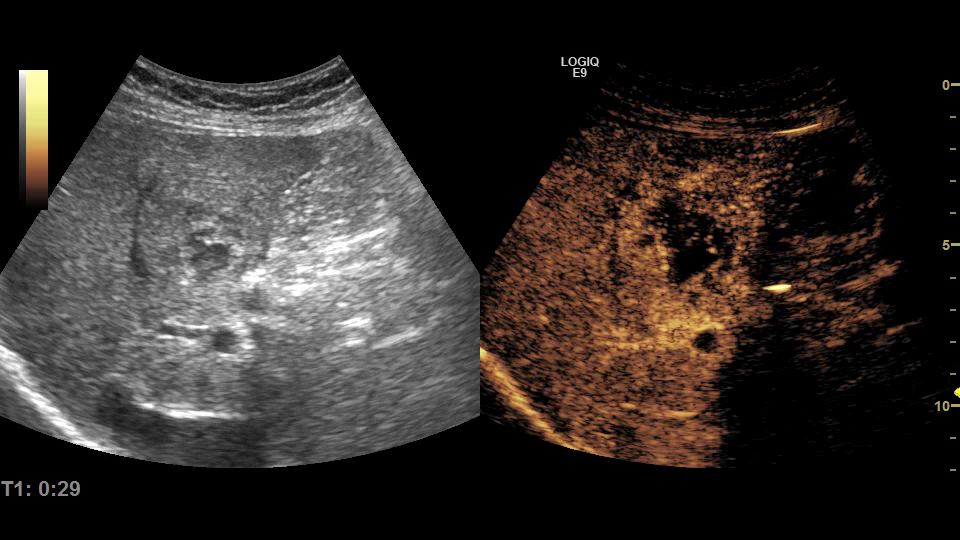
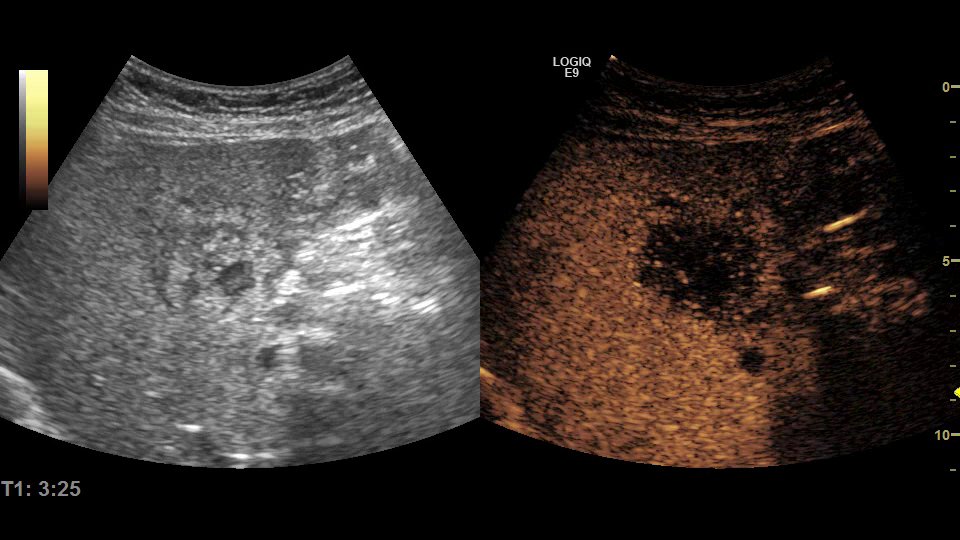
> iCCC (Fig. 3 – ring-like hyperenhancement & Fig. 4 – early wash-out)
are described in the table below:
| HEPATOCELLULAR CARCINOMA (Movie 1) |
CHOLANGIOCARCINOMA (Movie 2) |
|
| ARTERIAL PHASE | – hyperenhancing, homogeneous / heterogeneous, with areas of necrosis | – hyperenhancing, rim like enhancement |
| PORTAL-VENOUS PHASE | – iso-enhancing / hypoenhancing – slow wash-out (> 1 minute) | – hypoenhancing – fast wash-out (< 1 minute) |
| LATE PHASE | – hypoenhancing / iso-enhancing , no wash-out | – hypoenhancing / complete wash-out |
The features seen during CEUS are influenced by size, degree of differentiation, and surrounding liver parenchyma, and in practice there are multiple variations from typical appearances.
- The degree of differentiation:
– Poorly differentiated HCCs can exceptionally show a much faster wash-out (<60 seconds). The changes occurring in tumor microvasculature during the process of carcinogenesis can be the basis of this observation – the reduction of the number of tumoral sinusoids, with the acceleration of blood flow. A fast wash-out in the case of HCC (10-30 sec after contrast injection) is associated with tumor microinvasion and aggressive forms of HCC.
– On the other hand, well-differentiated HCCs may not show a wash-out phenomenon – secondary to a similar blood volume between the HCC and the surrounding parenchyma. - Tumor size – inhomogeneous enhancing in arterial phase in the case of large HCC (> 5 cm) secondary to areas of necrosis.
Increasing performance of CEUS in the differential diagnosis between HCC and CCC
- Considering the late wash-out phenomenon in the case of HCC – it is necessary to follow the lesions for longer time (7-8 min), possibly re-administrating the contrast agent.
- Quantitative analysis – automatic plotting of ICT curves (Time Intensity Curves) provides additional details on tumor perfusion and indicates significantly decreased values of perfusion parameters associated with portal venous and late phases (mTTI, FT) in iCCC compared to HCC.
- Particular regard to the clinical picture, laboratory tests, as well as the ultrasound appearance as a whole – liver parenchyma, biliary tract and vascular system.
| HEPATOCELLULAR CARCINOMA | CHOLANGIOCARCINOMA | |
| BIOLOGICAL | AFP (alpha-fetoprotein) |
CA 19-9 |
| ULTRASOUND | Tumor invasion in the portal vein – thrombus that expands the lumen, hyperenhancing in the arterial phase, with wash-out in the portal-venous or late phase. | Intrahepatic bile duct dilatations – transonic structures parallel to the branches of the portal vein> *spider look -in incidence visualizing the bifurcation of the portal vein. |