See other cases
Upper GI bleed – OTSC
History :
A 72-year-old man with a history of right ureteral neoplasm (G2/G3 urothelial carcinoma) with lung metastases, undergoing palliative chemotherapy (last session 4 days previously), presented with coffee-ground emesis and black, soft, shiny stools, with onset of 48 hours. Claims NSAID use in the past 10 days for epigastric pain.
Clinical & biological :
Altered general condition, intense pallor, BP = 72/43 mmHg, HR = 117 bpm, abdomen sensitive to palpation in the upper abdomen, melena.
Biological – hemoglobin = 4 g/dL
Imaging :
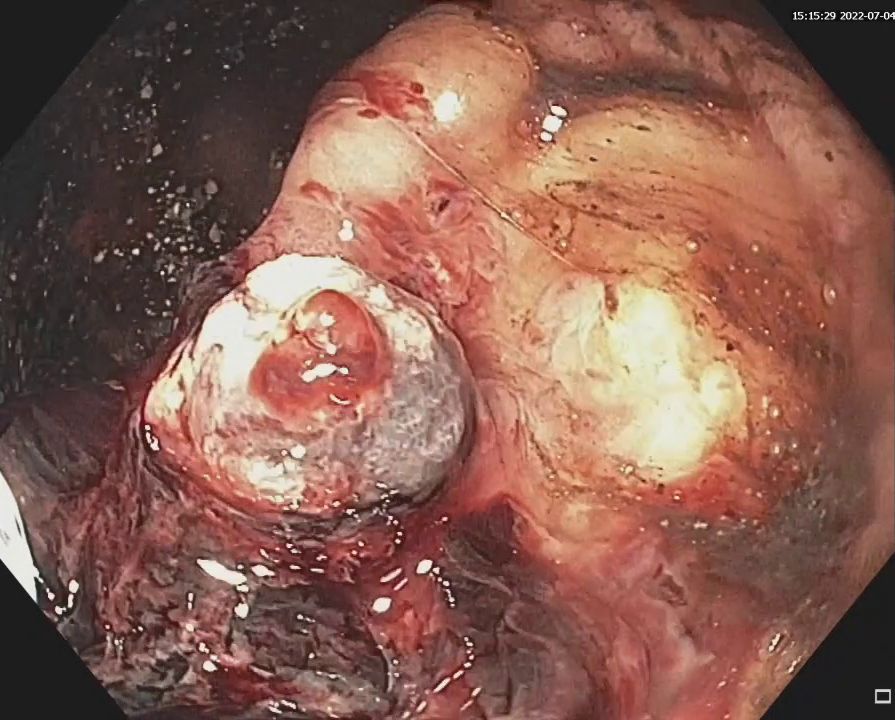
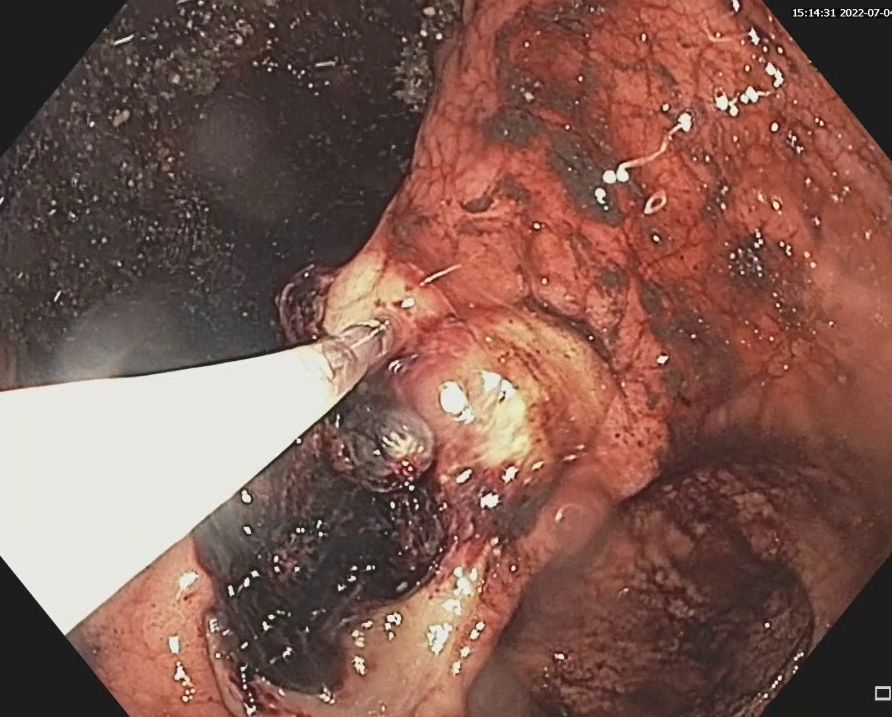
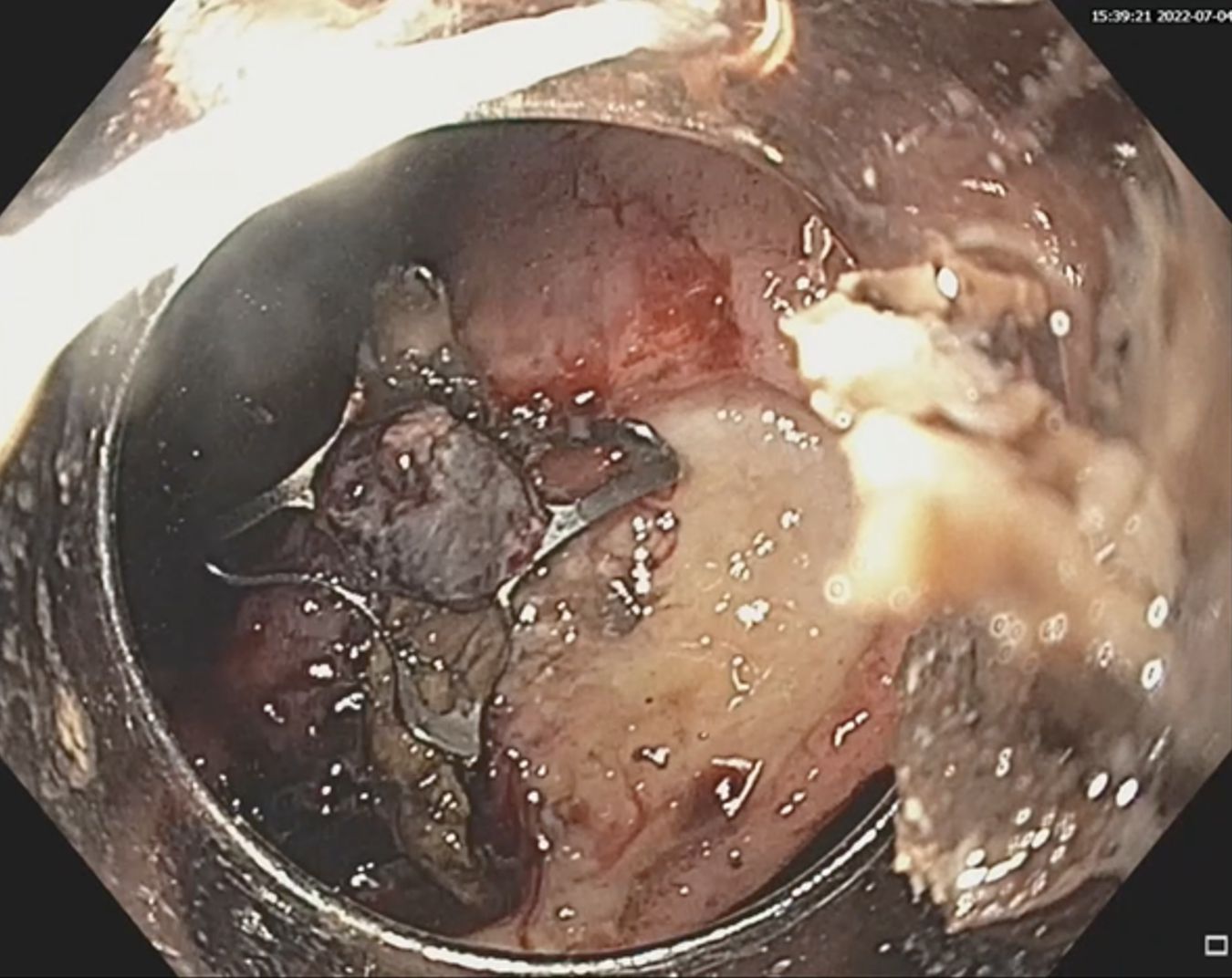
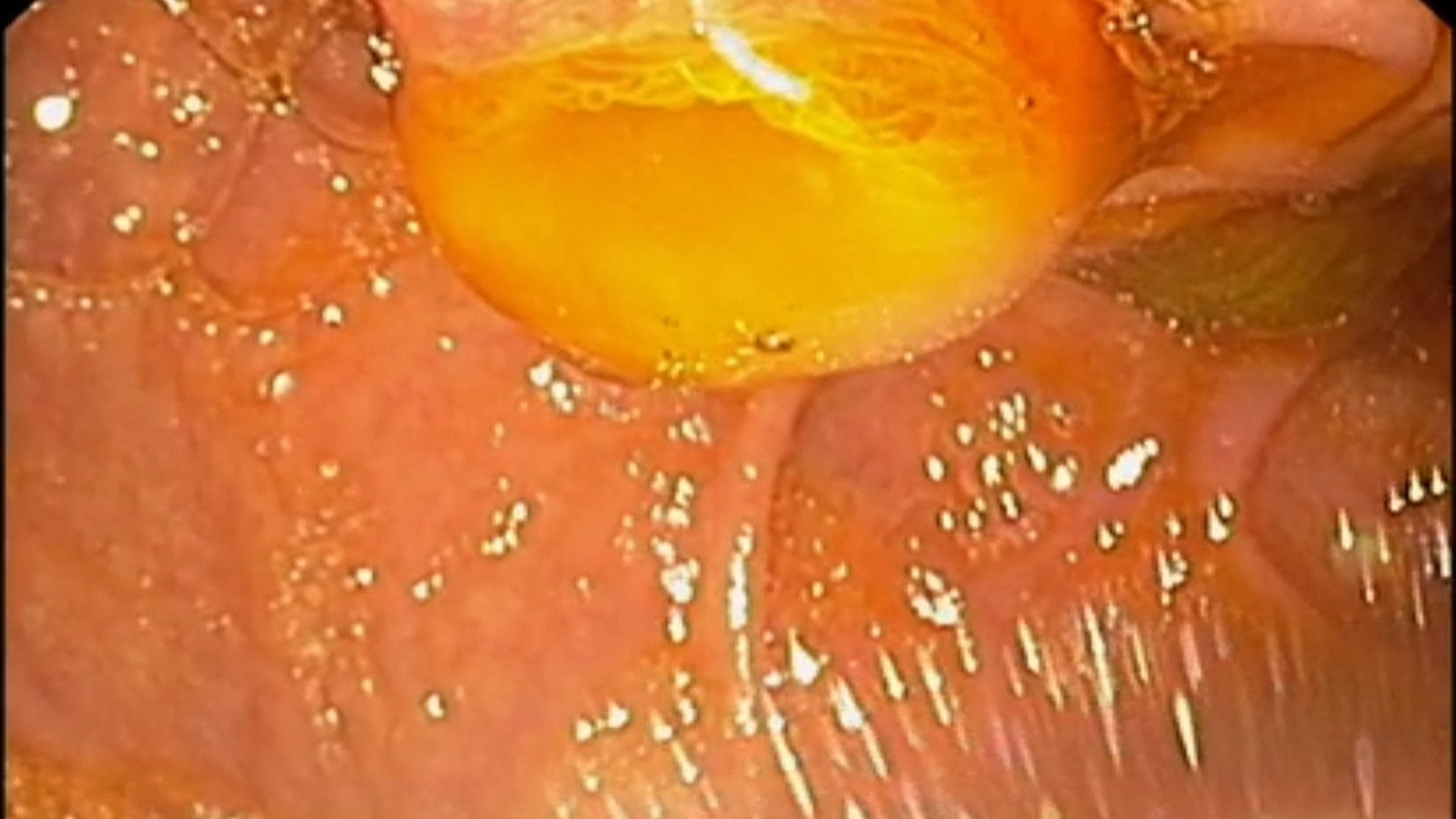
Upper GI endoscopy revealed an approximately 35 mm, deep ulcer at the gastric angle, with the crater covered with a large clot. After removing the clot by lavage, a large vessel is visualized (Forrest IIA). The second endoscopy, performed 5 days later in the context of rebleeding, revealed the same lesion (Figure 1). Approximately 10 mL of 1:10 000 diluted epinephrine was injected to achieve hemostasis and an over-the-scope clip (OTSC) was placed over the visible vessel (Figure 2, Movie 1).
Diagnostic :
Upper gastrointestinal bleeding from Forrest IIA gastric ulcer.
Discussion :
Typically, gastric or duodenal ulcers with a visible vessel (Forrest IIA) should receive endoscopic hemostasis by standard methods – electrocoagulation/placing hemoclips, with or without epinephrine injection. In the present case, taking into account the appearance of the lesion and the clinical context of the patient (altered general condition, hemodynamic instability, severe anemia), it was considered that there is a major risk of re-bleeding that is difficult or impossible to control endoscopically by the usual methods. Thus, endoscopic hemostasis was postponed to avoid a possible emergency surgical intervention in a biologically unbalanced patient with altered general condition. The evolution was initially favorable, with the improvement of the general condition and the improvement of the hemodynamic parameters. Five days later, the patient had a recurrent bleeding , with hemodynamic instability and significant deterioration. Upper GI endoscopy was performed and an over-the-scope clip was placed over the visible vessel, with a favorable subsequent evolution.
Conclusion :
The case illustrates a difficult situation – obtaining endoscopic hemostasis in the case of a deep, fibrous, large gastric ulcer, with a visible voluminous vessel, in a patient with severe upper GI bleeding, hemodynamically unstable, with severe anemia.
References :
1. Gralnek IM, Stanley AJ, Morris AJ et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2021. Endoscopy 2021; 53: 300-332
2. Kobara H, Mori H, Nishiyama N et al. Over-the-scope clip system: A review of 1517 cases over 9 years. J Gastroenterol Hepatol 2019; 34: 22-30.
3. Wedi E, von Renteln D, Gonzalez S et al. Use of the over-the-scope-clip (OTSC) in non-variceal upper gastrointestinal bleeding in patients with severe cardiovascular comorbidities: a retrospective study. Endosc Int Open 2017; 5: E875-E882.