See other cases
Splenic artery and celiac trunk aneurysms in a patient with portal hypertension
History :
Pacient cunoscut cu HTP segmentară, splenomegalie, cu un episod de HDS prin ruptura de varice esofagiene (bandate in 2010), se prezintă pentru evaluare clinică și ecografică.
Clinical & biological :
Clinic: șeft upper abdominal mild pain
Biologic: hemoglobin: 7.2 g/dl, serum iron: 13 microg/dl, ferritin: 18.4 ng/mL
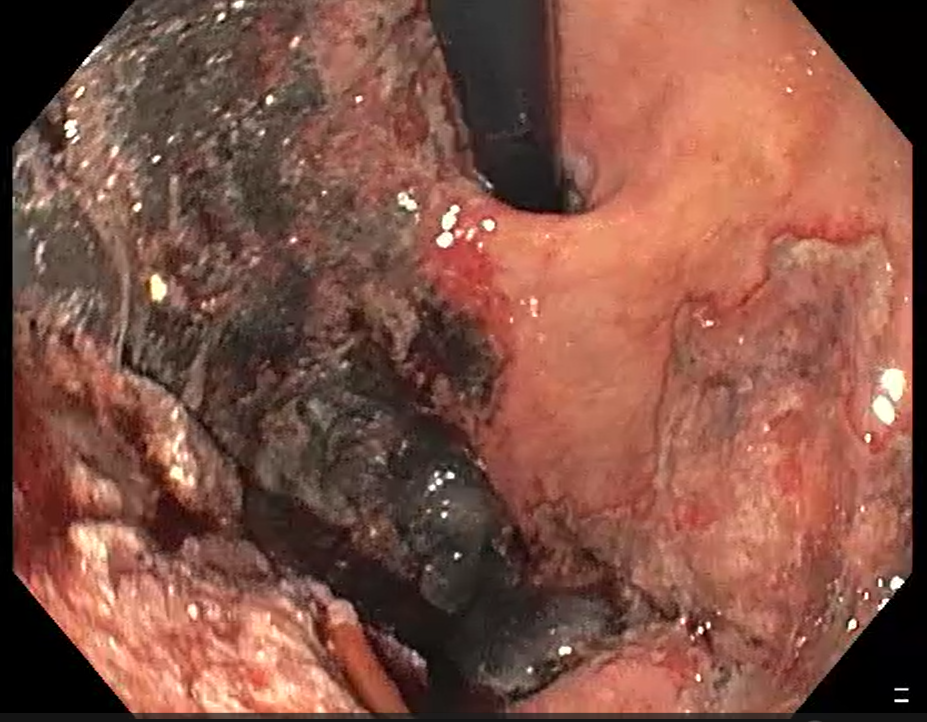
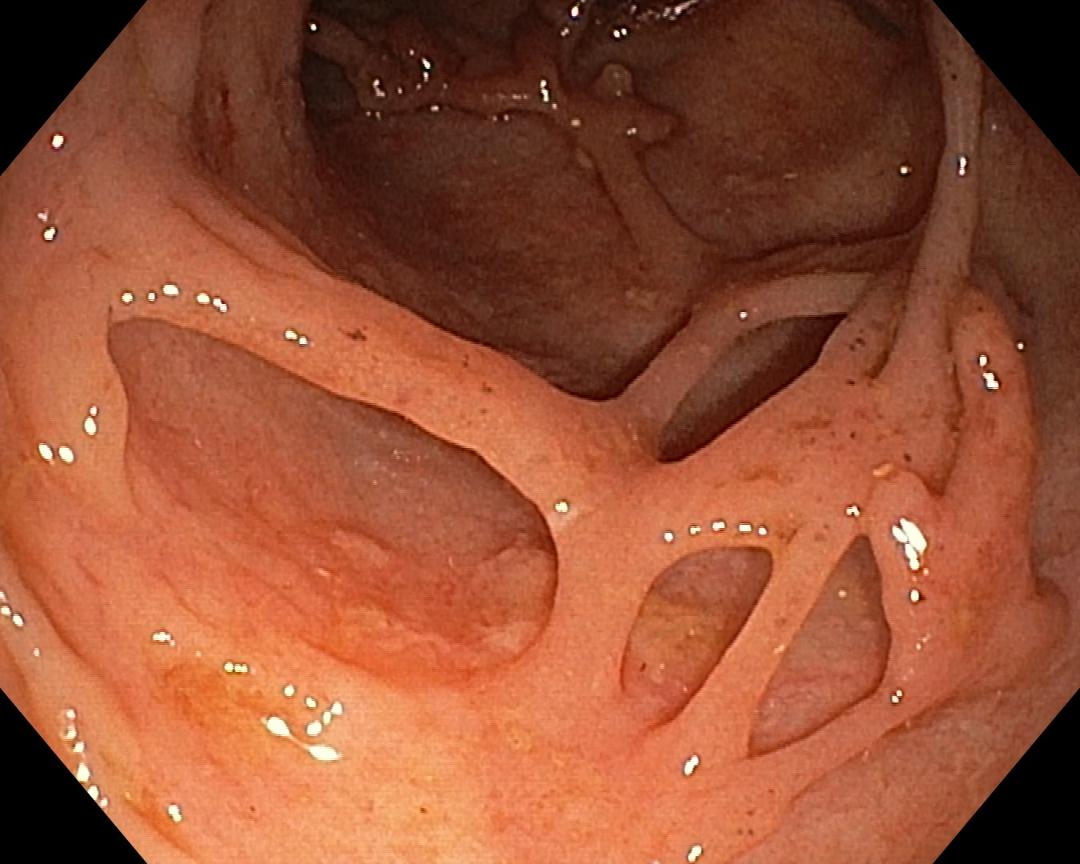
Imaging :
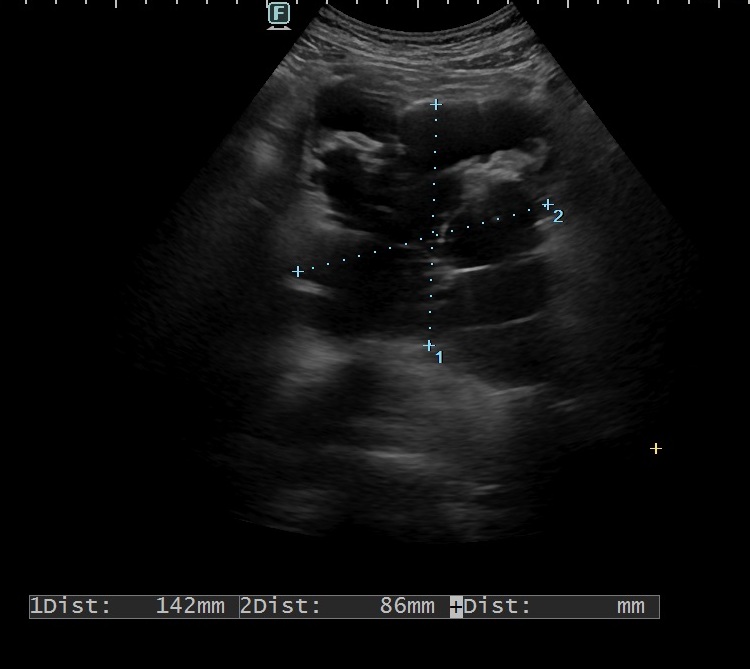
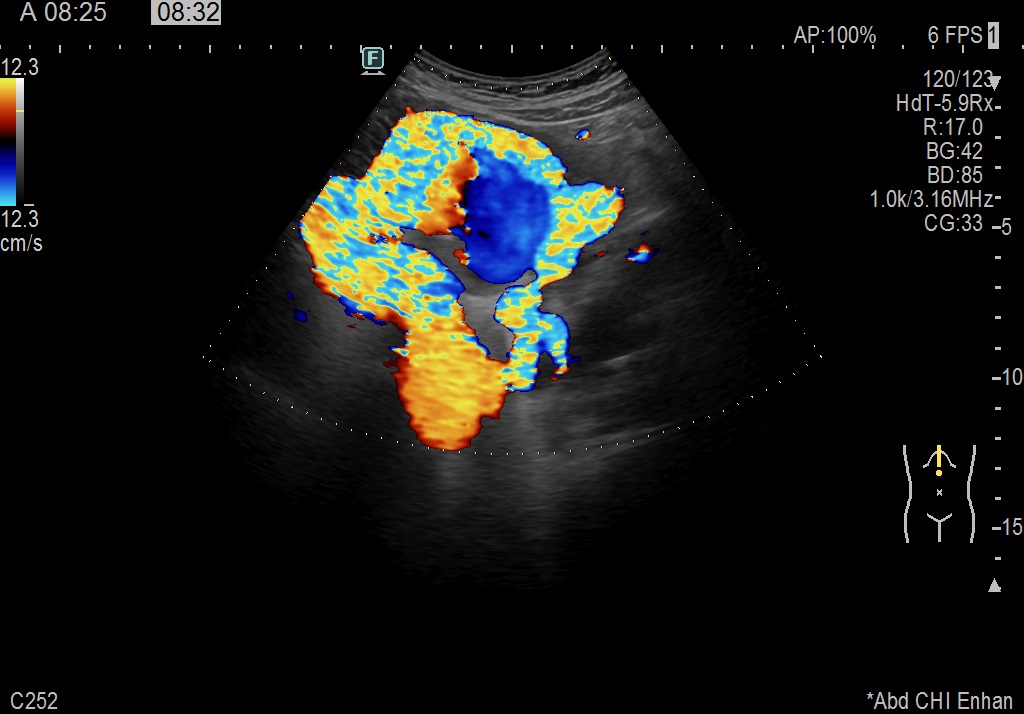
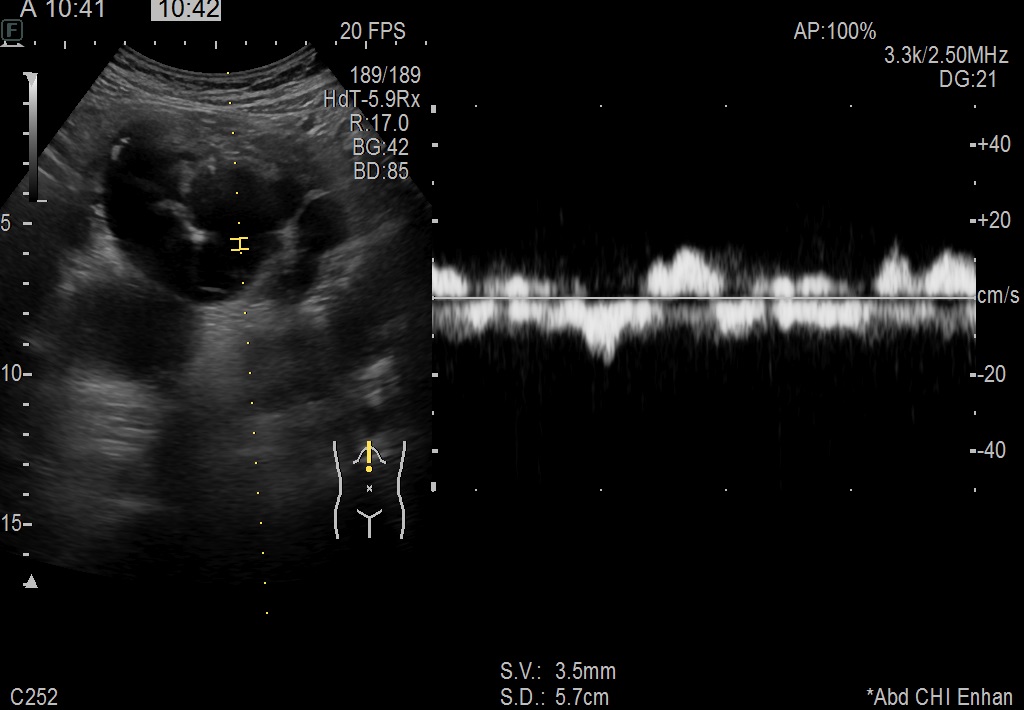
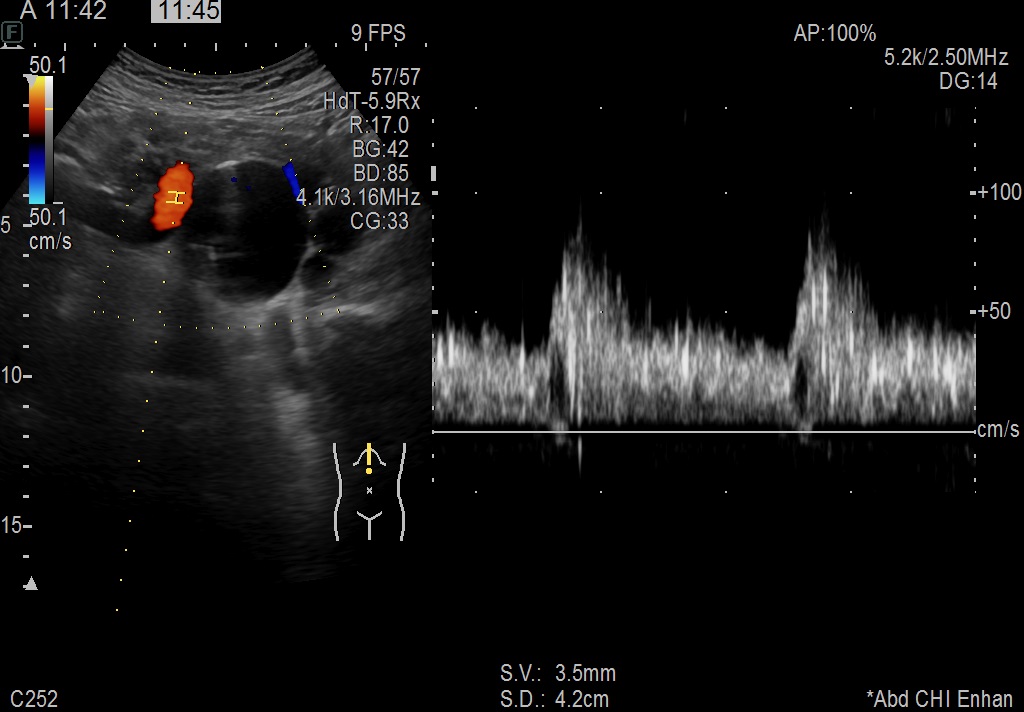
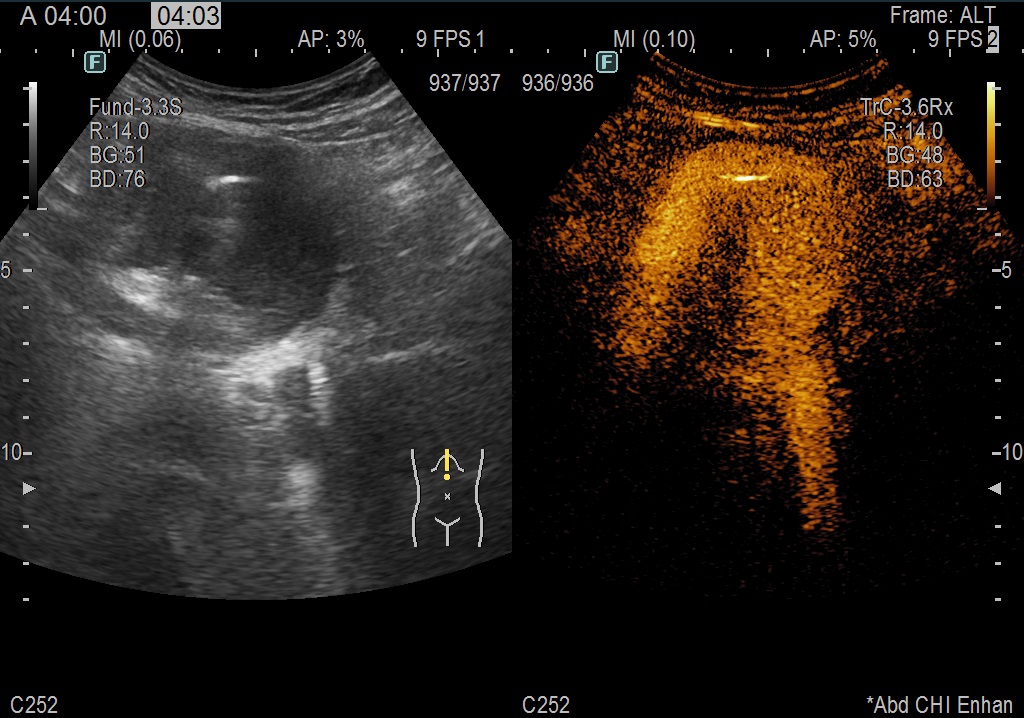
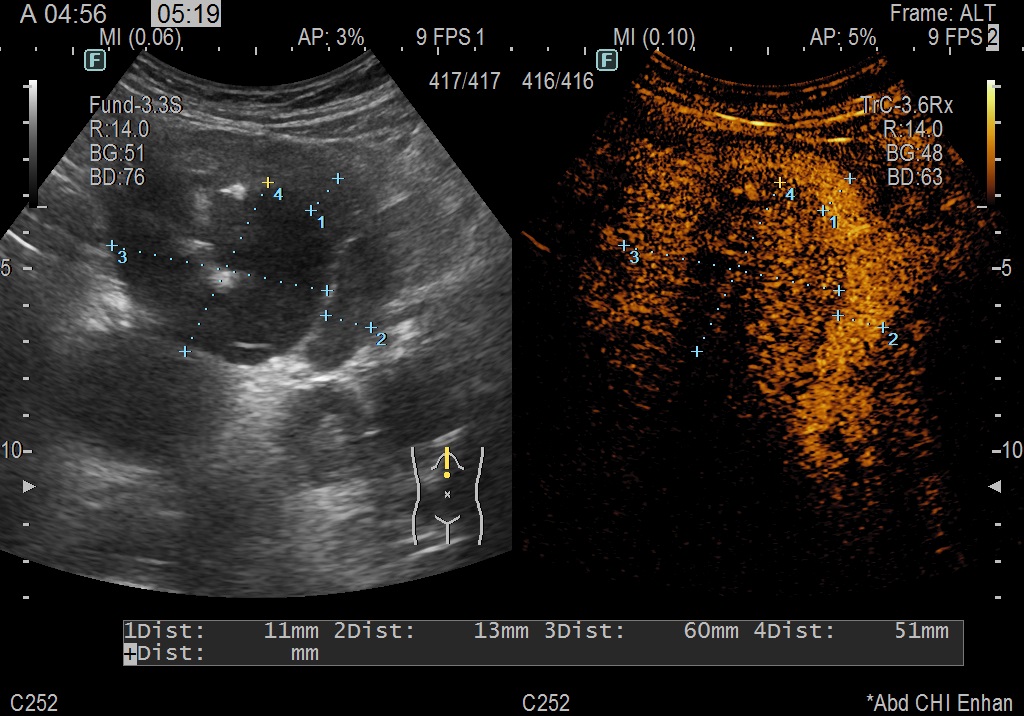
Abdominal ultrasound: in the right hepatic lobe, prerenal arterio-venous fistula, possibly resulting from a complicated liver biopsy puncture (2002), splenomegaly with large venous dilatations in hilum, no free liquid detected.
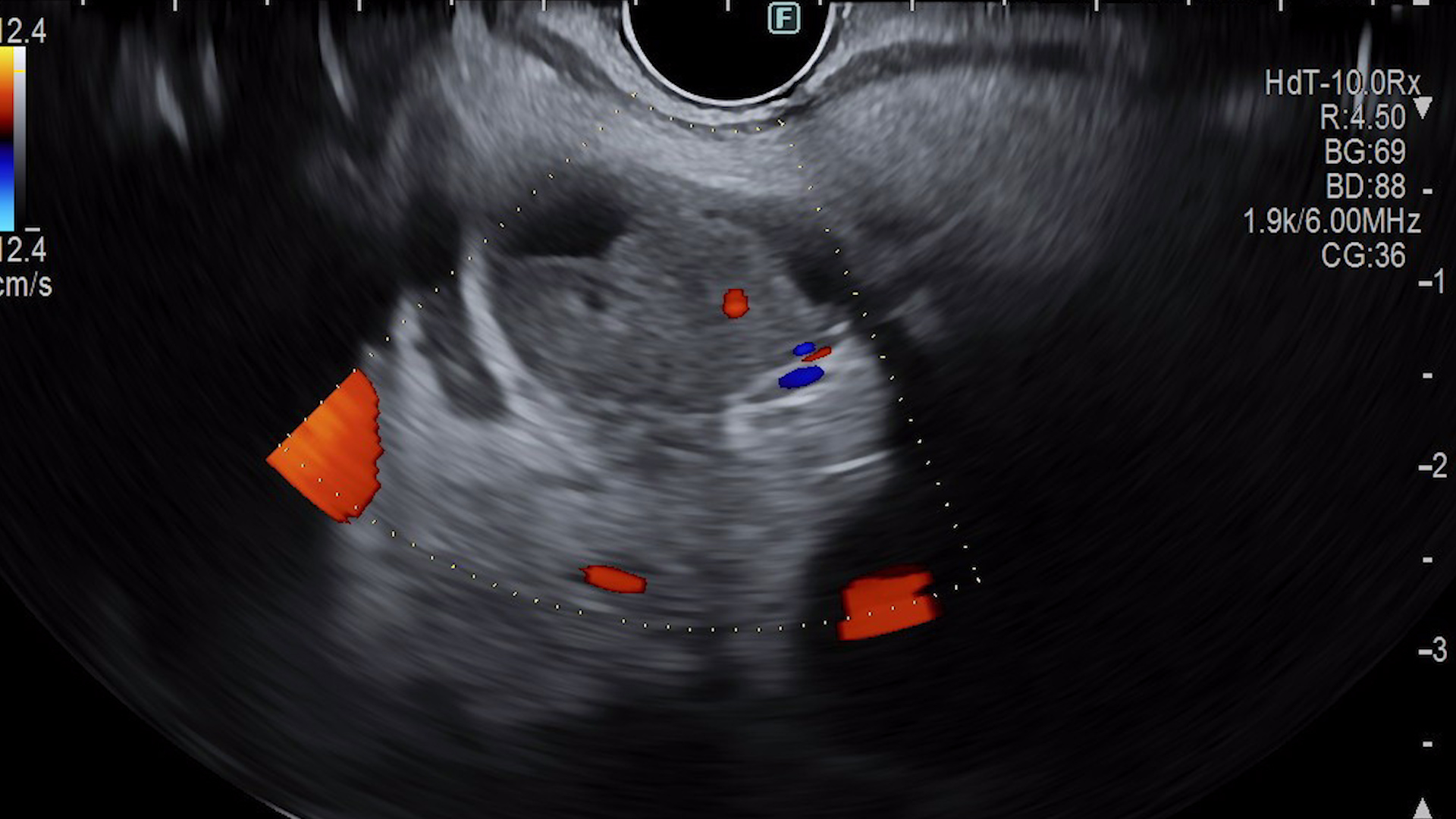
CEUS: In the epigastric region, complex pseudoaneurysmal structure (approx. 7 x 7 cm) with mixed internal flow (arterial + venous), requiring further imaging.
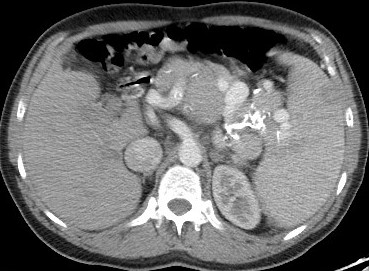
Abdominal and thoracic CT scan with contrast: Mildly dysmorphic liver. CT signs of portal hypertension. Voluminous porto-systemic collateral circulation. Dilated celiac trunk, main emergences and hepatic arterial vascular axes , splenic artery (with multiple segmental fusiform aneurysms of maximum 22 mm). Portal vein trunk with caliber within normal limits (approx. 14 mm) with chronic, calcified parietal thrombosis. Voluminous porto-systemic collateral circulation, some with an aneurysmal appearance and parietal calcifications, in the upper abdomen, extending superiorly, paraesophageal and draining to the superior vena cava level via the azygos vein (caliber 24 mm). Indirect signs of pulmonary hypertension and right heart overload secondary to collateral circulation.
Diagnostic :
Segmental portal hypertension with splenic artery and celiac trunk aneurysms.
Discussion :
The patient’s history, clinical presentation, and imaging findings suggest the presence of portal hypertension, which is localized to a specific segment of the liver. The arterio-venous fistula in the right hepatic lobe, possibly a result of a previous liver biopsy complication, could contribute to the portal hypertension and its associated complications. The patient’s history of esophageal varices rupture and subsequent banding in 2010 is consistent with portal hypertension, as well as splenomegaly and complex pseudoaneurysmal structure further support this diagnosis.
Splenic artery aneurysm is the most common type of visceral aneurysm, usually saccular and 2-4 cm in size. It’s more common in females and can be life-threatening if it ruptures, leading to severe hemorrhage. About 22% of cases are emergencies, with an 8.5% mortality rate. Treatment options include surgery, embolization, or stenting. The risk is higher for larger aneurysms (>5 cm), giant ones (>10 cm) having a 28% rupture risk and up to 40% mortality. Moreover, celiac trunk aneurysms are described more rearely and frequently show no symptoms. If symptoms do arise, they are typically vague and nonspecific. The most critical risk associated with these aneurysms is rupture, which can result in a mortality rate of up to 100%.
Treatment should be pursued for patients with symptomatic aneurysms, pregnant or in the reproductive age range, individuals with le-sions exceeding 2 cm, those experiencing progressively growing lesions, or patients with portal hypertension. While various treatment approaches exist, surgery is considered the optimal choice for addressing giant aneurysms.
Conclusion :
Overall, the patient’s condition requires a multidisciplinary approach involving gastroenterologists, hepatologists, and interventional radiologists to manage the segmental portal hypertension, its associated complications, and the potential underlying liver disease. Aneurysms of the splenic artery and celiac trunk are rare but with a high mortality rate, which is why the patient requires careful monitoring for possible complications.
References :
- Beksac K, Karakoc D. Multiple Giant Splenic Artery Aneurysms Causing Sinistral (Left-Sided) Portal Hypertension. Case Rep Gastrointest Med. 2016;2016:6278452. doi: 10.1155/2016/6278452.
- Rehman ZU. Multiple Giant Splenic Artery Aneurysms with Hypersplenism and Portal Hypertension: A Case Report. Ann Vasc Dis. 2019 Jun 25;12(2):250-252. doi: 10.3400/avd.cr.19-00021.
- Yakubovitch D, Halak M, Khaikin M, Silverberg D. Multiple splenic artery aneurysms in a patient with portal hypertension. Isr Med Assoc J. 2013 Jan;15(1):55-6.
- Giampaolo Carrafiello, Nicola Rivolta, Matteo Annoni, Federico Fontana, Gabriele Piffaretti. Endovascular repair of a celiac trunk aneurysm with a new multilayer stent. Journal of Vascular Surgery. 2011;54(4): 1148-1150.