See other cases
Recto-vaginal fistula (OTSC)
History :
We present the case of a 44-year-old woman with a history of total hysterectomy for a uterine mesothelial tumor (July 2023), complicated by an iatrogenic bowel perforation requiring segmental enterectomy. Her medical history was also notable for hiatal hernia and osteoporosis.
A few months after surgery, the patient developed vaginal passage of flatus and fecaloid discharge.
Imaging :
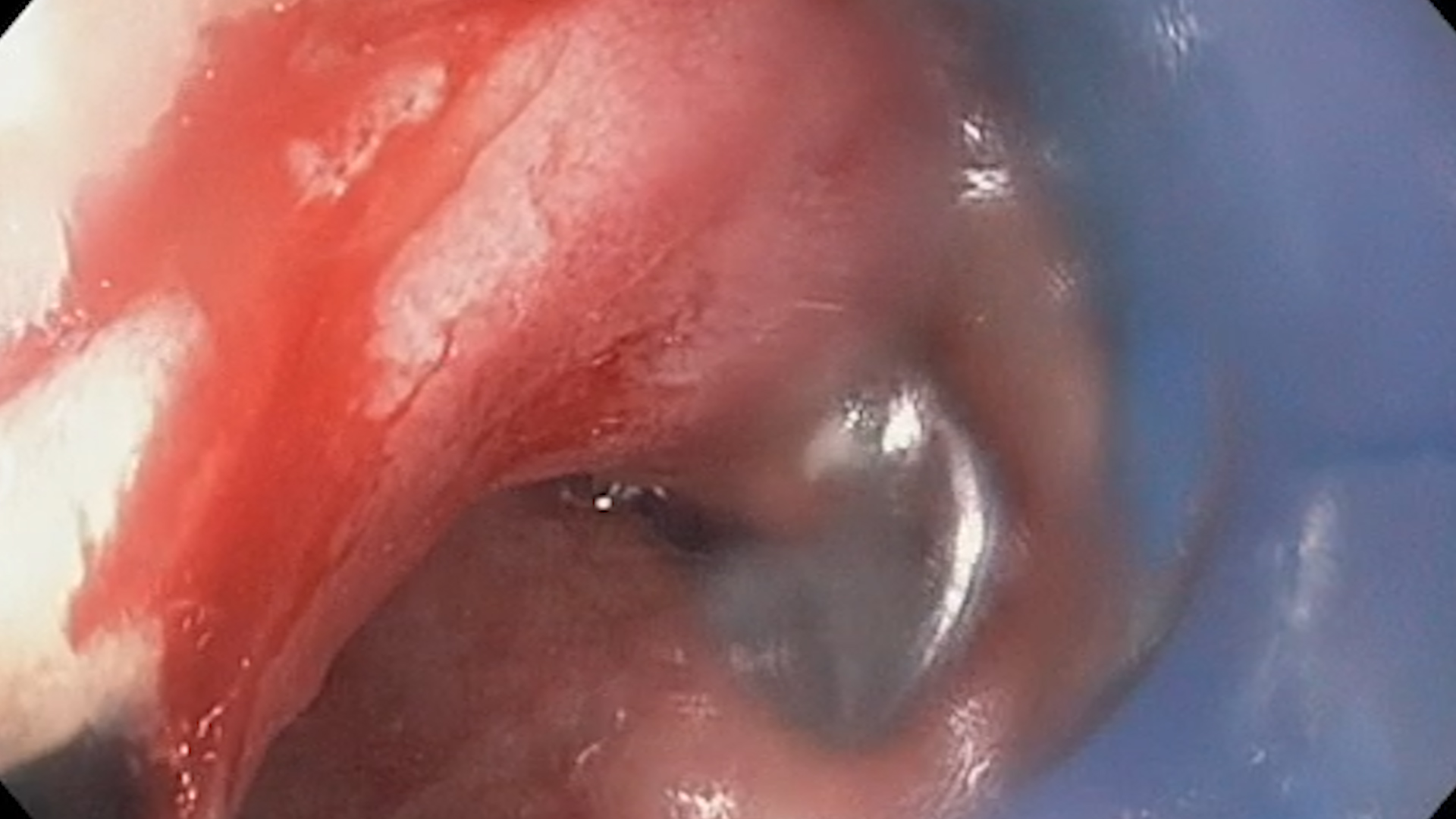
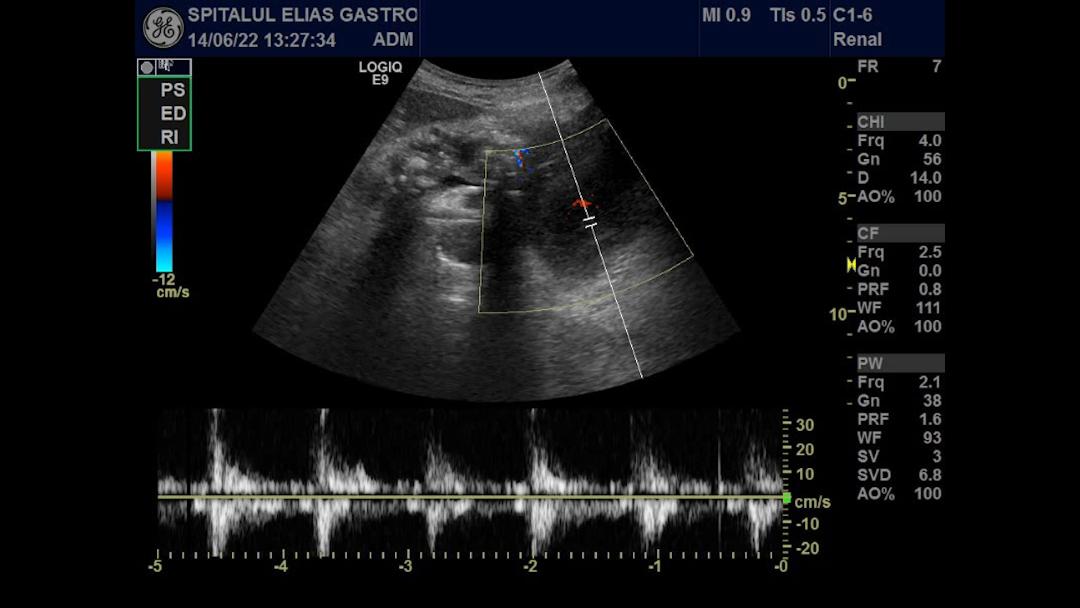
Pelvic MRI revealed an oblique fistulous tract extending from antero-superior to a postero-inferior, measuring approximately 2.1 mm in diameter. Multiple colonoscopic examinations were performed, the rectal opening of the fistula could not be successfully identified. Approximately two years later, the patient was re-evaluated, with surgical repair being considered if the rectal orifice remain undetected. During the initial colonoscopy, the fistulous opening could not be identified (Fig. 0). Given the fact that the fistula was readily identified during gynecological examination, a repeat evaluation using a Pipelle cannula was undertaken (Fig. 1-2).
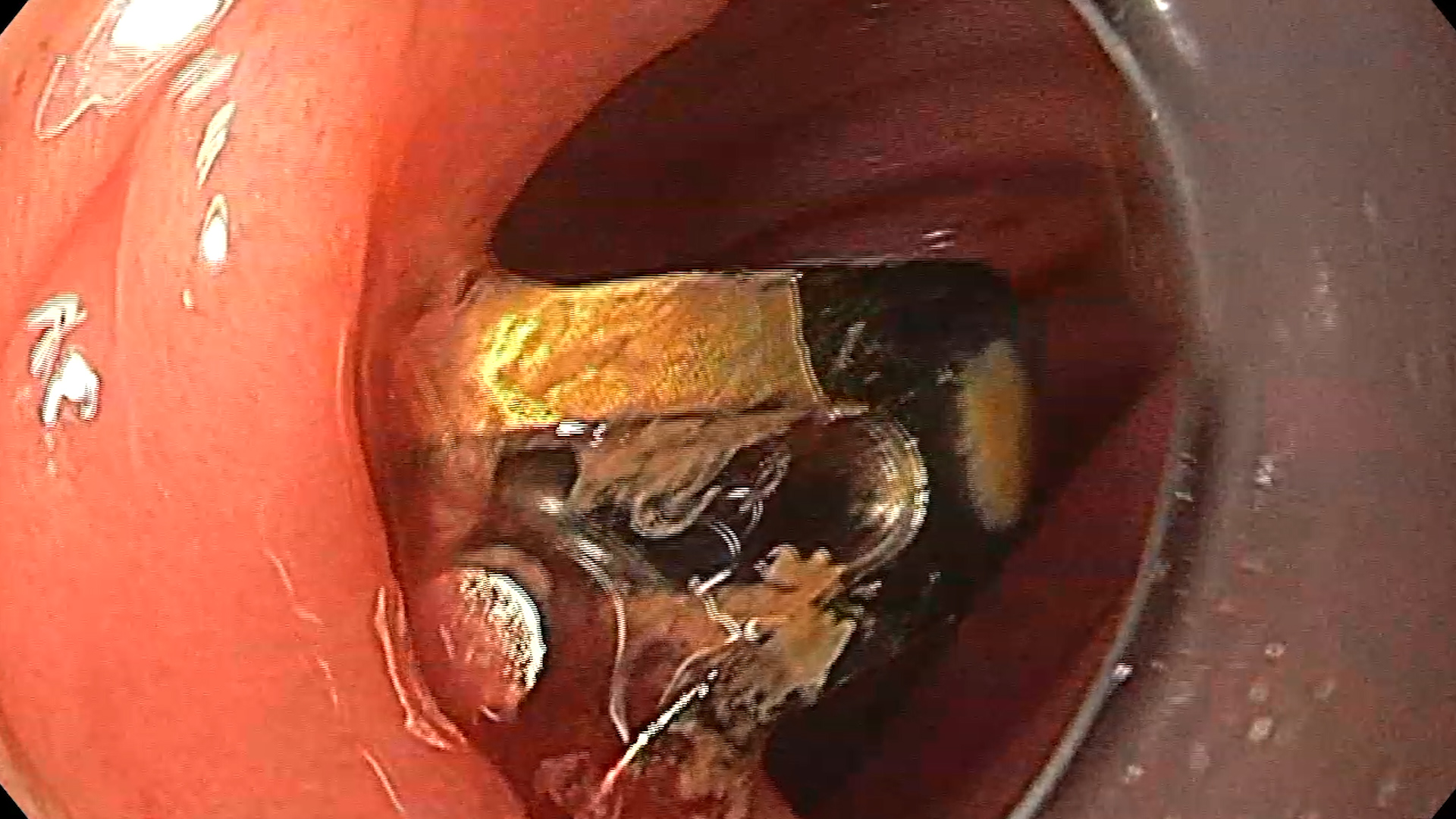
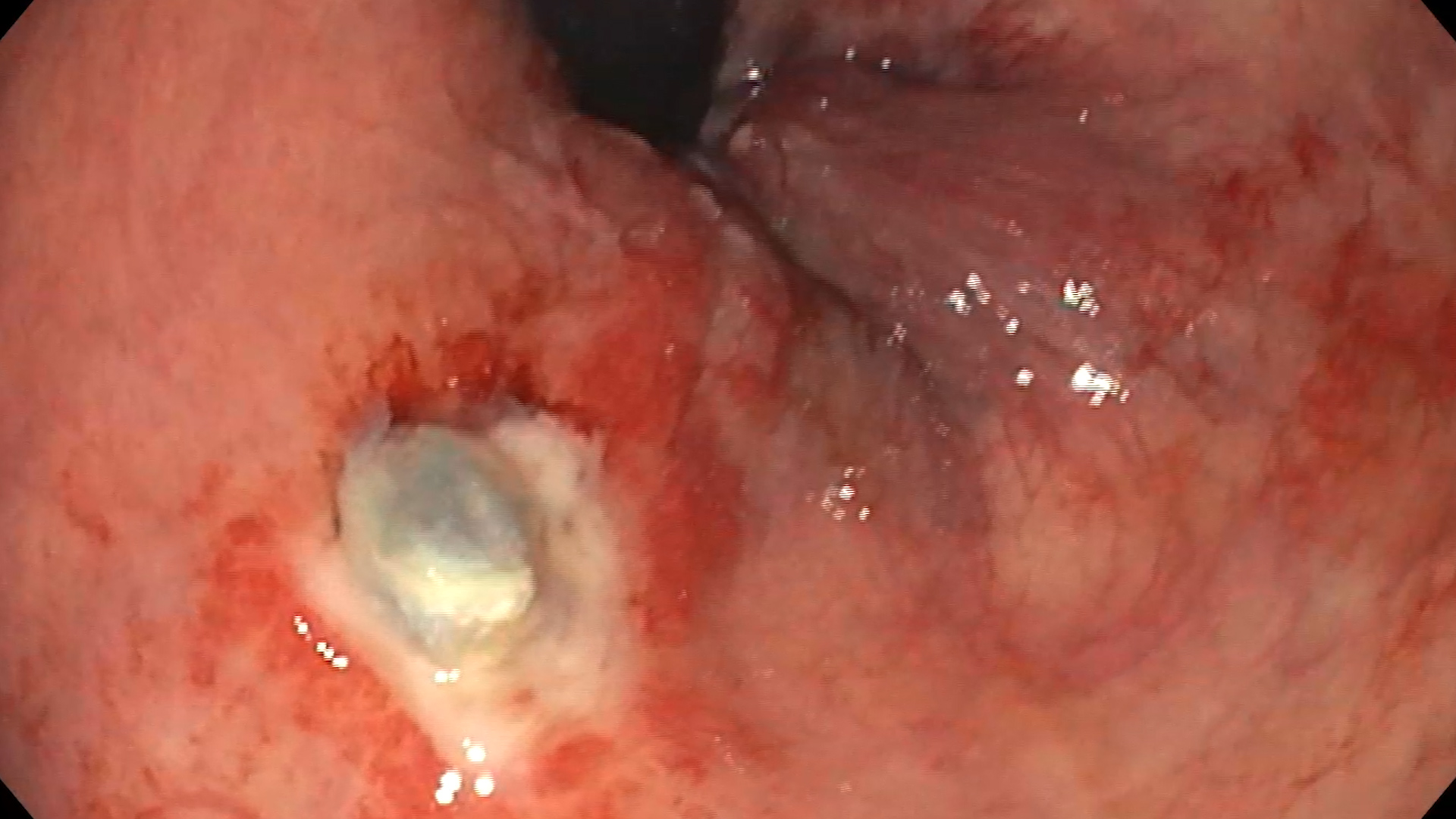
To accurately identify the rectal opening of the fistula, a combined sigmoidoscopic and gynecological examination was performed using the Pipelle cannula, with the endoscope in retroflexion. Following multidisciplinary discussion, endoscopic treatment with an over-the-scope clip (OTSC) was selected. Closure of the defect was achieved using the Dual Grasper device provided by the manufacturer (Ovesco®) (Fig. 3-5). Successful closure was confirmed intraprocedurally by instillation of methylene blue through the Pipelle cannula via the vaginal route, with no dye leakage observed into the intestinal lumen.
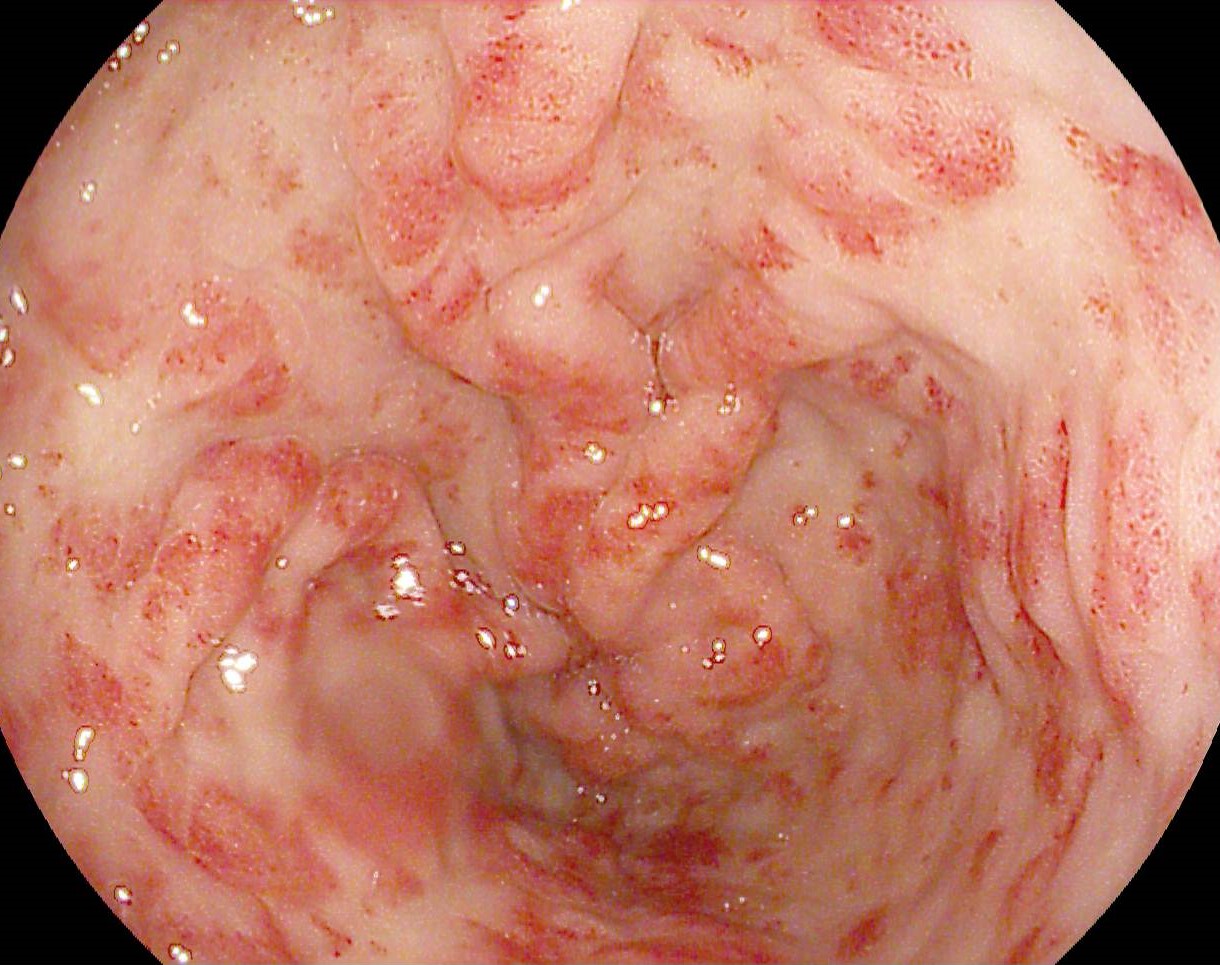
At the 6-month follow-up, the OTSC remained in situ (Fig. 6). The patient reported complete resolution of vaginal passage of feculent material and flatus.
Diagnostic :
- Chronic rectovaginal fistula – effective closure of the rectal orifice using an Ovesco® clip
- Status post total hysterectomy
- Status post segmental enterectomy
Discussion :
The first steps in the management of a rectovaginal fistula (RVF) include assessment of fistula size, location, and etiology, evaluation of the anal sphincter complex and surrounding tissues, thus classifying fistula as “simple” or “complex”, the presence of inflammation, a diverting stoma, previous repair attempts, or prior radiation therapy; and consideration of the patient’s overall condition and comorbidities.[1]
In this case, the defect met the criteria for a simple fistula because of its small orifice, low location and benign etiology (obstetric surgical trauma).
Current guidelines recommend initial conservative management of RVFs, including local wound care, baths, debridement when necessary, antibiotics in cases of infection, and stool-bulking fiber supplementation, generally for a period of 3–6 months. When conservative treatment fails, non-surgical therapeutic options include self-expandable metallic stents, fibrin glue, and endoluminal clipping[1].
Definitive closure of the rectovaginal fistula was achieved using an over-the-scope clip (OTSC, Ovesco®). This system provides durable tissue apposition by remaining attached to the mucosa for an extended period and by capturing a larger amount of tissue than conventional through-the-scope clips, thereby increasing the likelihood of sustained fistula closure.
Since the first RVF closure using the OTSC® Proctology system was reported by Prosst in 2015, studies have demonstrated variable success rates ranging from 40% to 93%. The heterogeneity of reported outcomes may be attributable to the scarcity of high-quality evidence and to the technical expertise required for OTSC deployment, given the relatively recent introduction of this technique into clinical practice. A small number of cases involving persistent fistulas at the end of follow-up and abscess formation requiring drainage have also been reported.[2–4]
Conclusion :
Endoscopic closure of RVF using the OTSC system is a promising minimally invasive option, particularly in carefully selected patients. Treatment efficacy appears to depend on fistula duration, with better outcomes reported in recent lesions than in chronic fistulas.
References :
- Maeda K, Wada N, Shida A. Treatment of Rectovaginal Fistula. J Anus Rectum Colon. 2023 Apr 25;7(2):52-62. doi: 10.23922/jarc.2023-007. Erratum in: J Anus Rectum Colon. 2023 Jul 25;7(3):224. doi: 10.23922/jarc.E004. PMID: 37113583; PMCID: PMC10129357.
- Tong Y, Trilling B, Sage PY, Girard E, Faucheron JL. Short-term outcomes of the over-the-scope clip proctology system for rectovaginal fistula repair: a prospective study. Tech Coloproctol. 2019 Mar;23(3):245-249. doi: 10.1007/s10151-019-01948-5. Epub 2019 Apr 1. PMID: 30937645.
- van Vledder MG, Doornebosch PG, de Graaf EJ. Transanal endoscopic surgery for complications of prior rectal surgery. Surg Endosc. 2016 Dec;30(12):5356-5363. doi: 10.1007/s00464-016-4888-8. Epub 2016 Apr 8. PMID: 27059974.
- Zeng YX, He YH, Jiang Y, Jia F, Zhao ZT, Wang XF. Minimally invasive endoscopic repair of rectovaginal fistula. World J Gastrointest Surg. 2022 Sep 27;14(9):1049-1059. doi: 10.4240/wjgs.v14.i9.1049. PMID: 36185557; PMCID: PMC9521462.