See other cases
GAVE syndrome
History :
A 85-year-old patient with chronic kidney disease presents for dyspnea on exertion and, affirmatively, with melena.
Clinical & biological :
Clinical: Pallor, dyspnea on exertion. Paraclinical: hemoglobin = 5.9 g / dL, serum iron 12 ng / mL, ferritin 6 ng / mL.
Imaging :
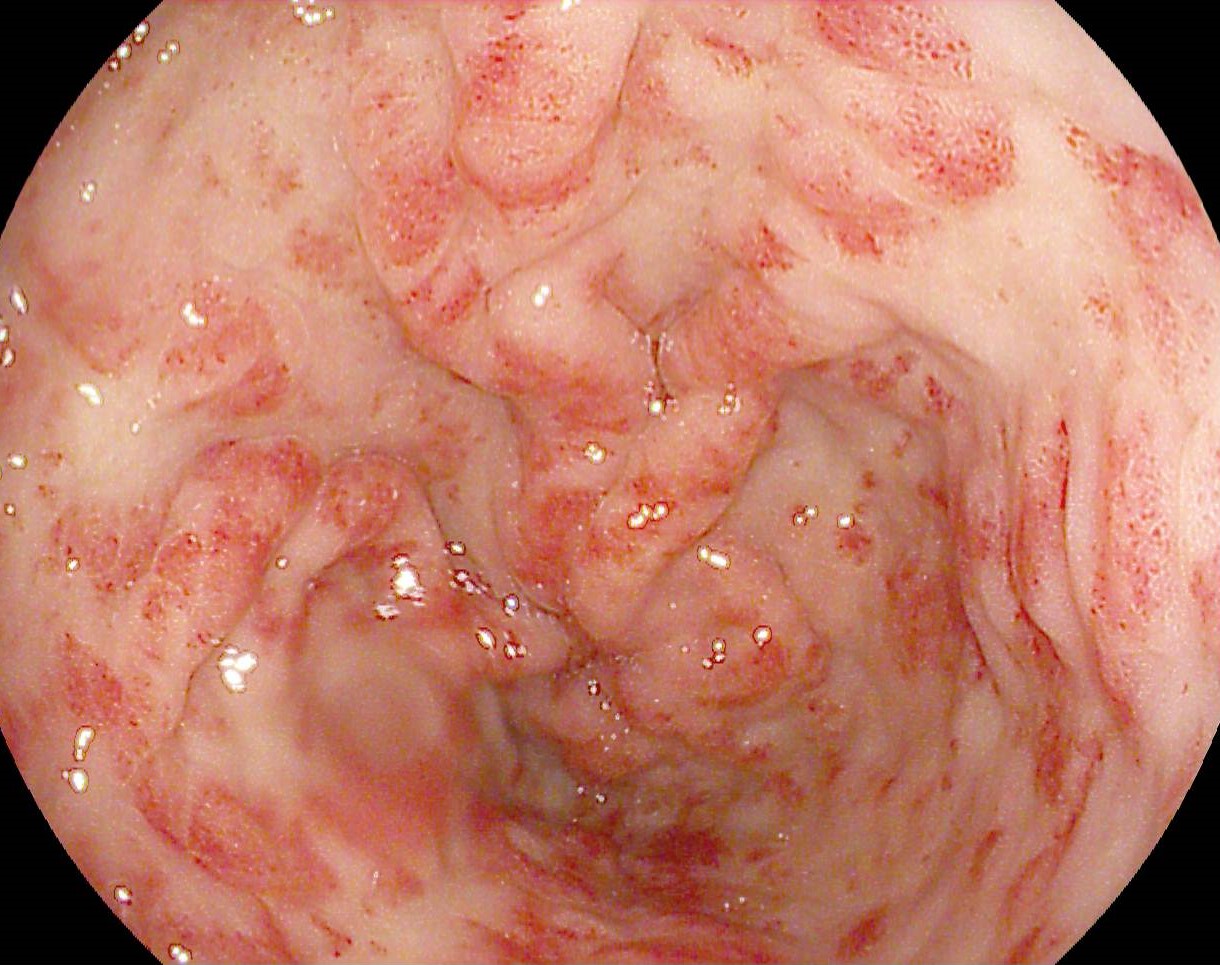
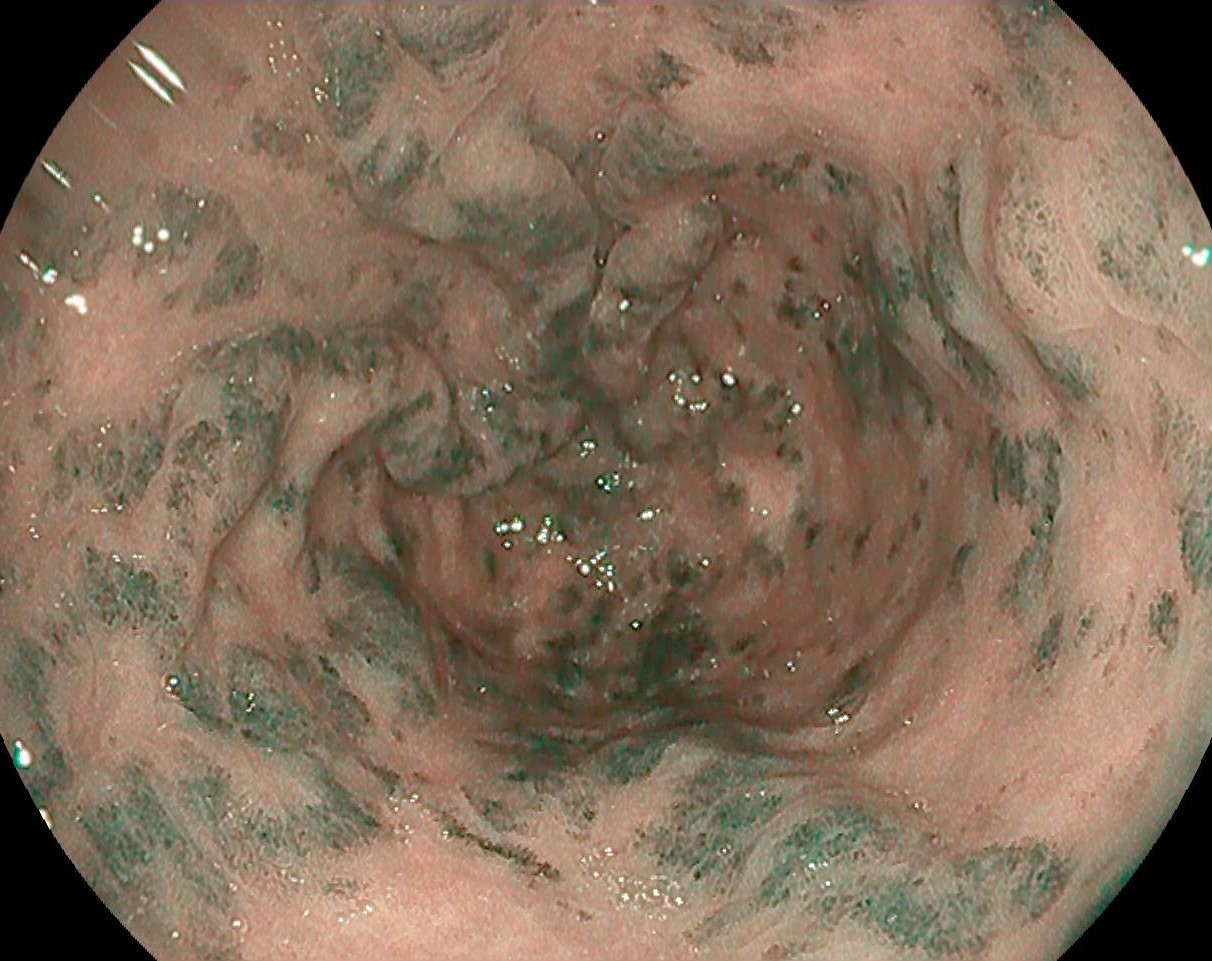
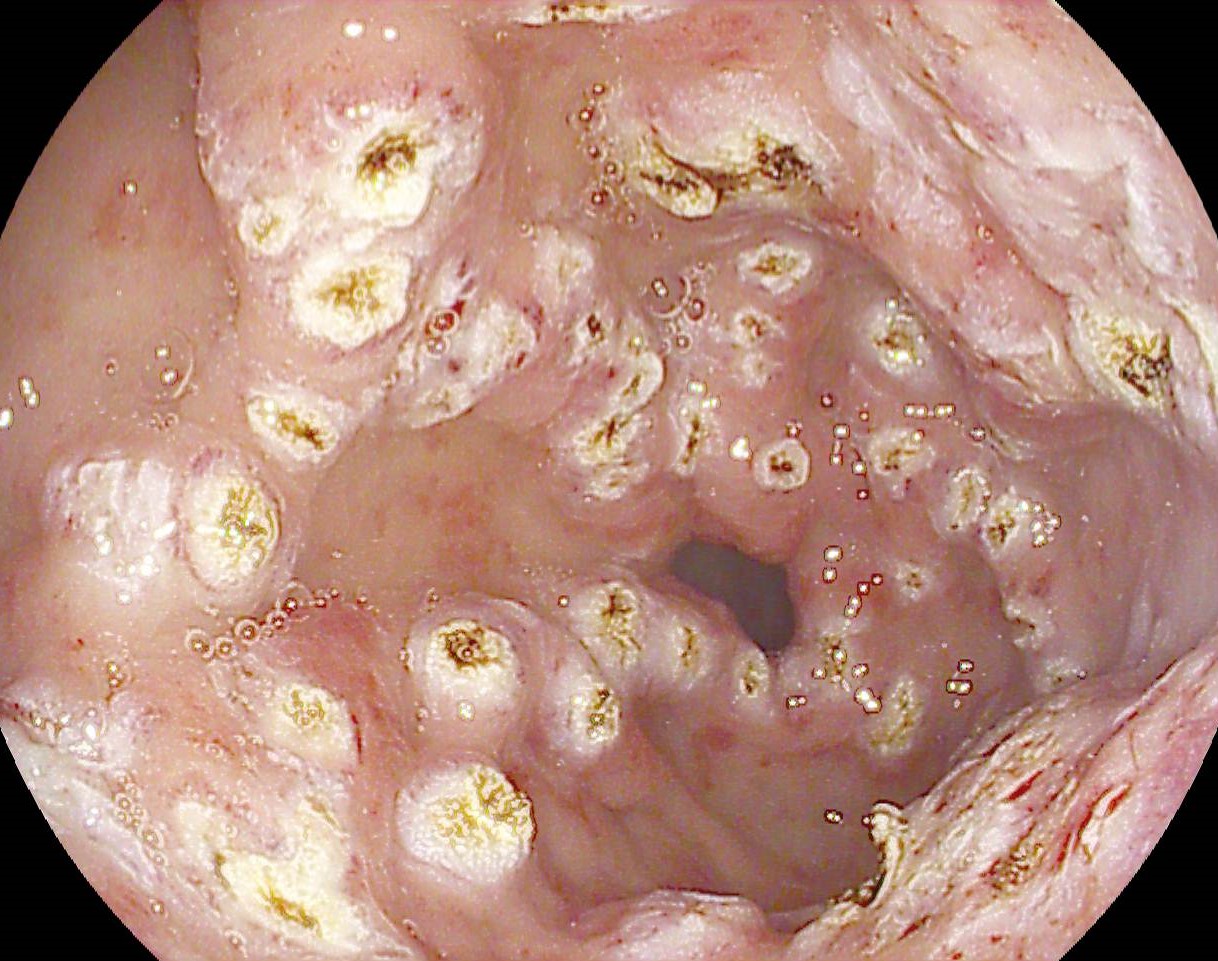
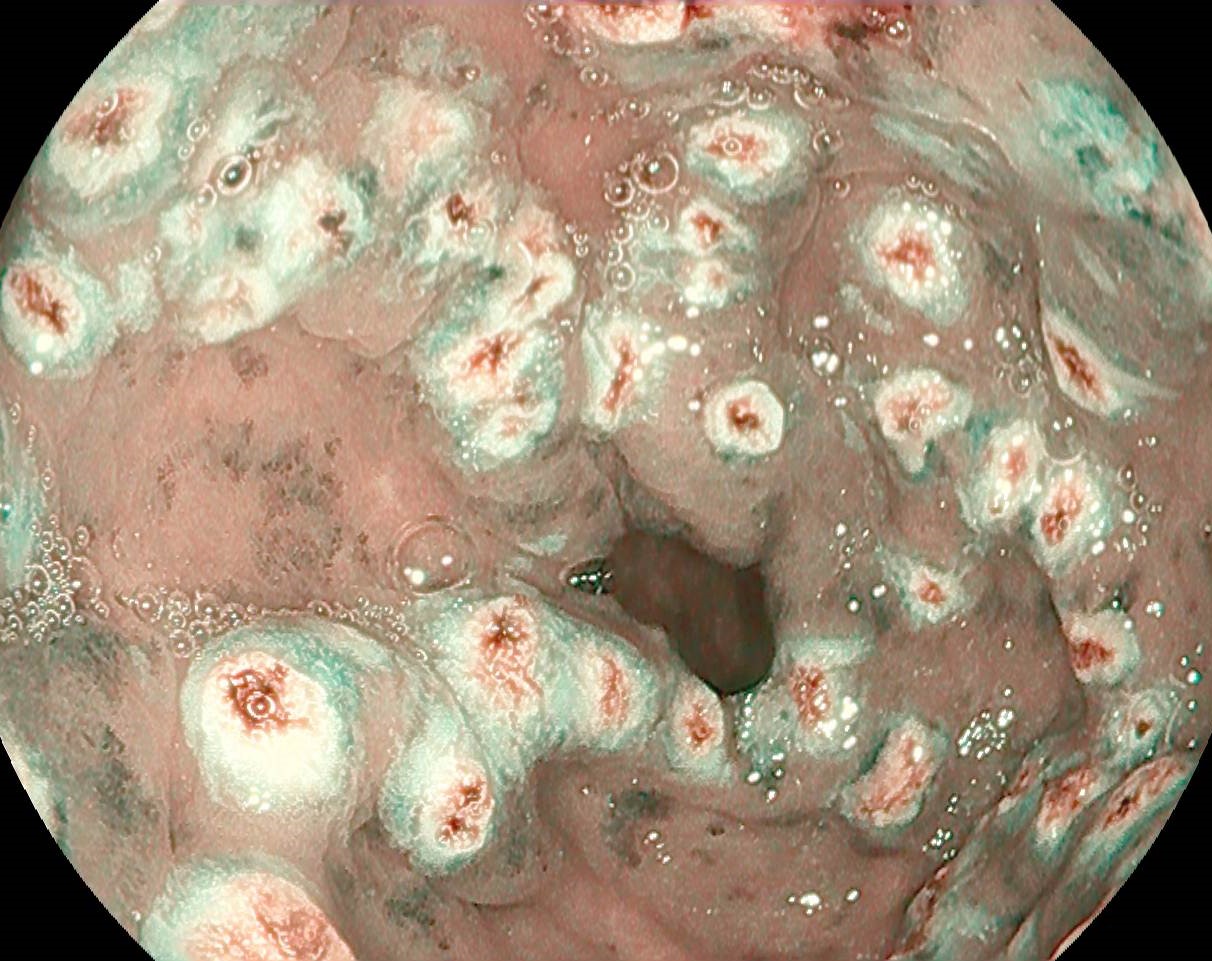
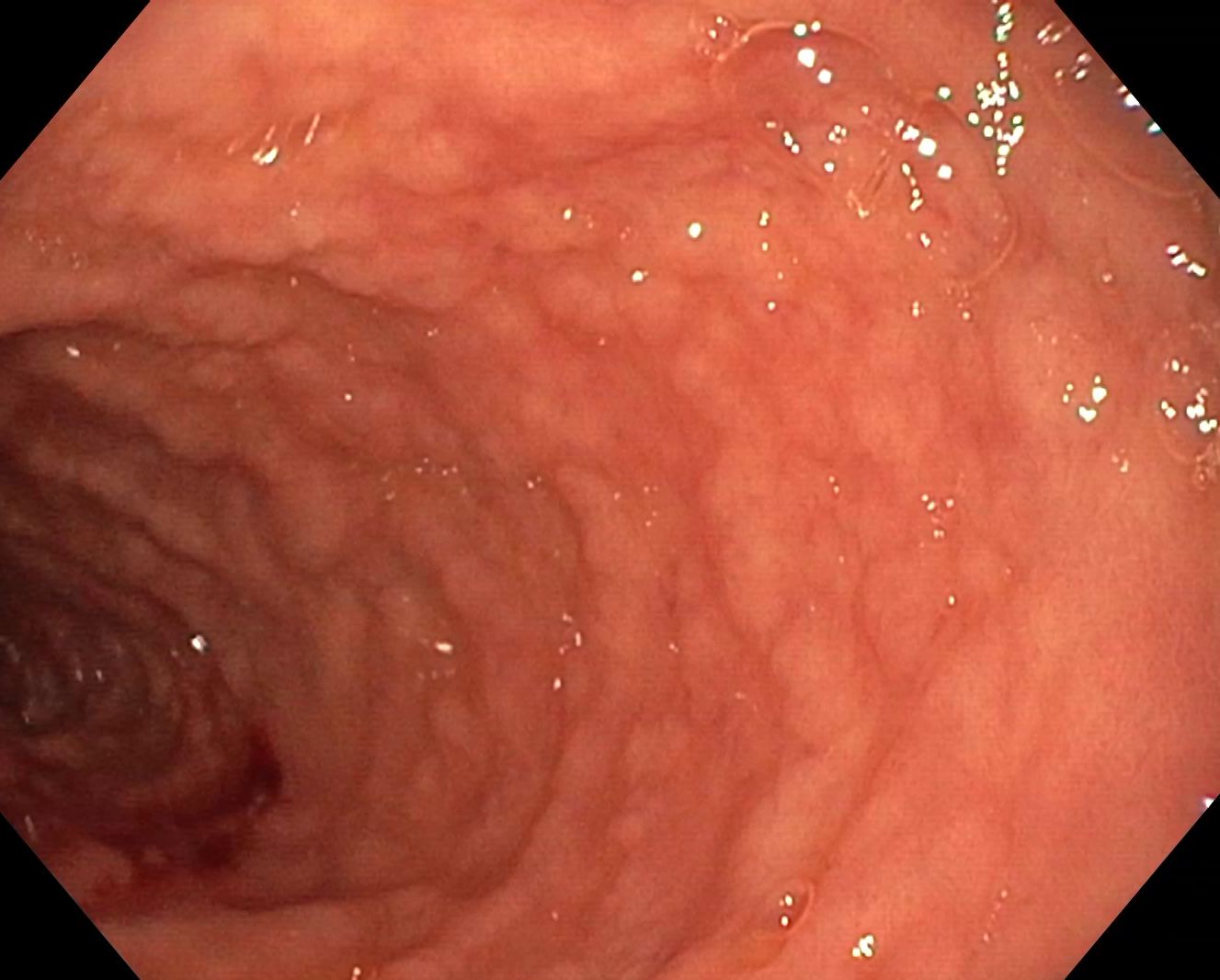
Upper GI endoscopy revealed multiple angiectasias disseminated in the antrum suggestive for GAVE syndrome (“watermelon stomach”), visualized in iSCAN 1 and OE (optical enhancement) mode (Figure 1-2, Movie 1). The lesions were coagulated with argon plasma (APC) without bleeding at the end of the procedure (Figure 3-4, Movie 2).
Diagnostic :
GAVE syndrome (“watermelon stomach”)
Discussion :
GAVE syndrome (“watermelon stomach”) is a rare acquired vascular condition that causes iron deficiency anemia, with variable onset from occult bleeding to signs and symptoms of upper gastrointestinal bleeding (manifested as hematemesis and melena). It is commonly associated with autoimmune diseases, liver cirrhosis, chronic kidney disease and cardiovascular disease. The pathogenesis is complex and includes impaired antral motility, with mucosal trauma and submucosal fibromuscular hyperplasia, followed by capillary dilation. Treatment is complex and includes medical options (corticosteroids, estrogen-progesterone in postmenopausal women, octreotides, tranexamic acid), endoscopic procedures (argon plasma coagulation (APC), elastic band ligation, radiofrequency ablation, cryotherapy), less often surgical treatment (antrectomy). APC is a non-contact thermal procedure, which allows superficial coagulation in the mucosa, with low risk of perforation, being considered the current treatment of choice in GAVE syndrome.
Conclusion :
The detailed examination allows to establish the correct technique of coagulation with argon plasma and the eradication of vascular lesions in GAVE syndrome.
References :
1. Kichloo A, Solanki D, Singh J, et al . Gastric Antral Vascular Ectasia: Trends of Hospitalizations, Biodemographic Characteristics, and Outcomes With Watermelon Stomach. Gastroenterology Res. 2021; 14: 104-111.
2. Hsu WH, Wang YK, Hsieh MS, et al. Insights into the management of gastric antral vascular ectasia (watermelon stomach). Therap Adv Gastroenterol 2018; 11: 1756283X17747471.
3. Zulli C, Del Prete A, Romano M, Esposito F, Amato MR, Esposito P. Refractory gastric antral vascular ectasia: a new endoscopic approach. Eur Rev Med Pharmacol Sci 2015; 19(21): 4119-22.
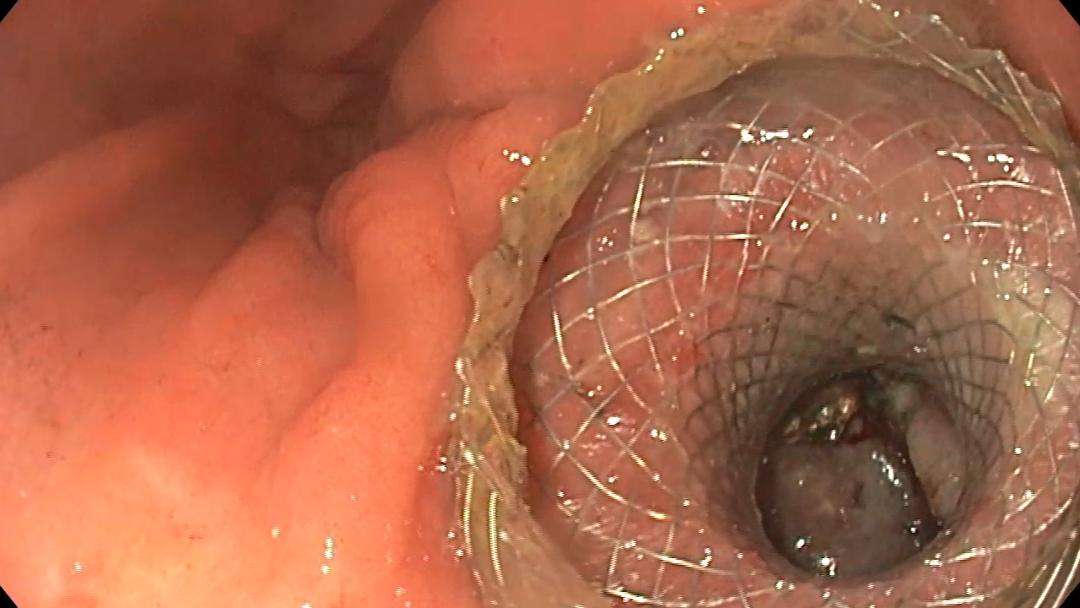
Plastic is fantastic: rescue drainage with plastic stents after LAMS drainage of a pancreatic pseudocyst
Endoscopic ultrasound, Endoscopy