See other cases
Gastric varices
History :
A 62-year-old male with known ethanolic liver cirrhosis and hepatocarcinoma with portal vein thrombosis presented with hematemesis and melena.
Clinical & biological :
Altered general state, pallor, spider telangiectasis on the anterior thorax, leg edema, abdomen distended by ascitic fluid, with periumbilical collateral circulation, liver and spleen non-palpable due to large amount of ascitic fluid.
Hemoglobin = 4.7 g/dL
Imaging :
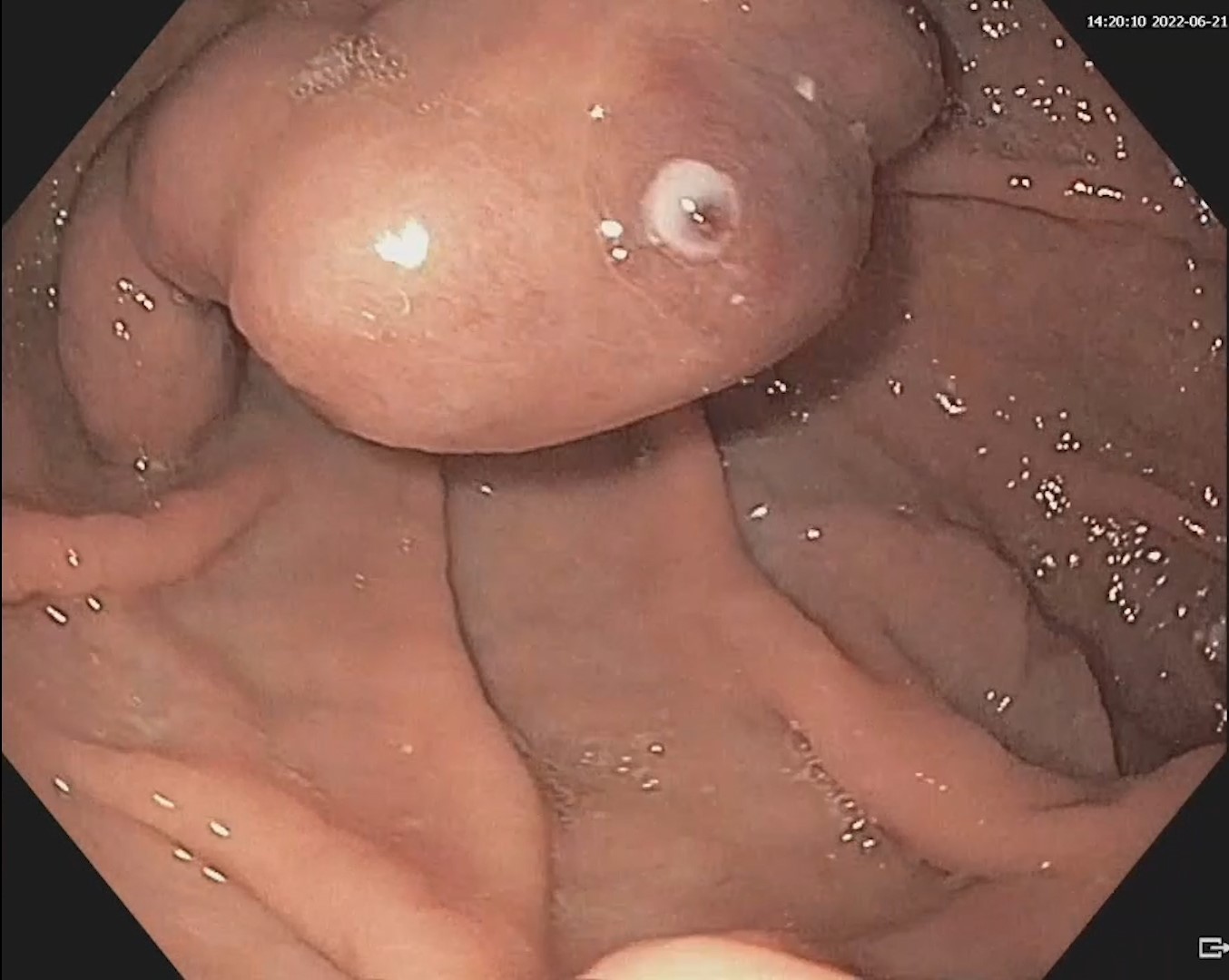
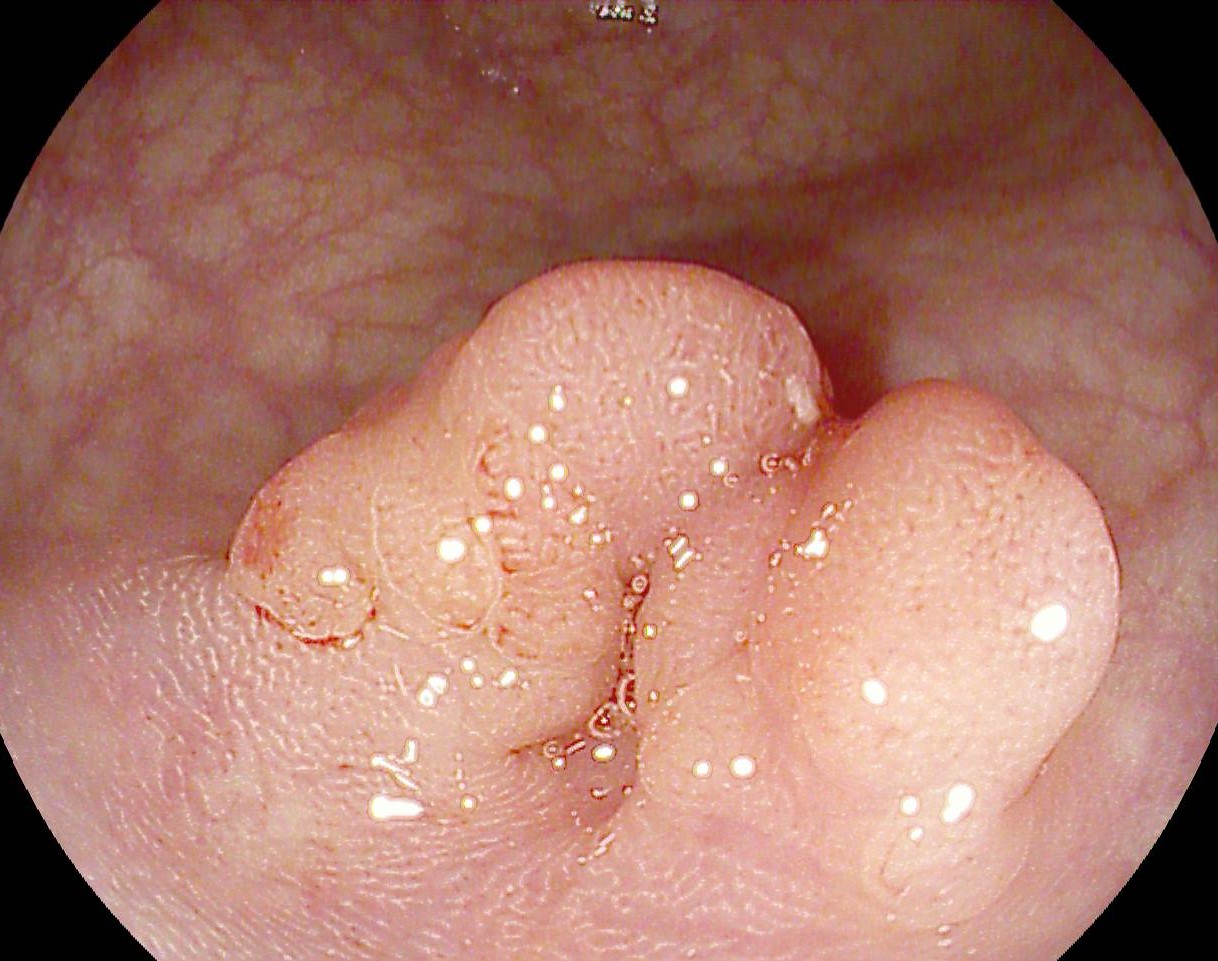
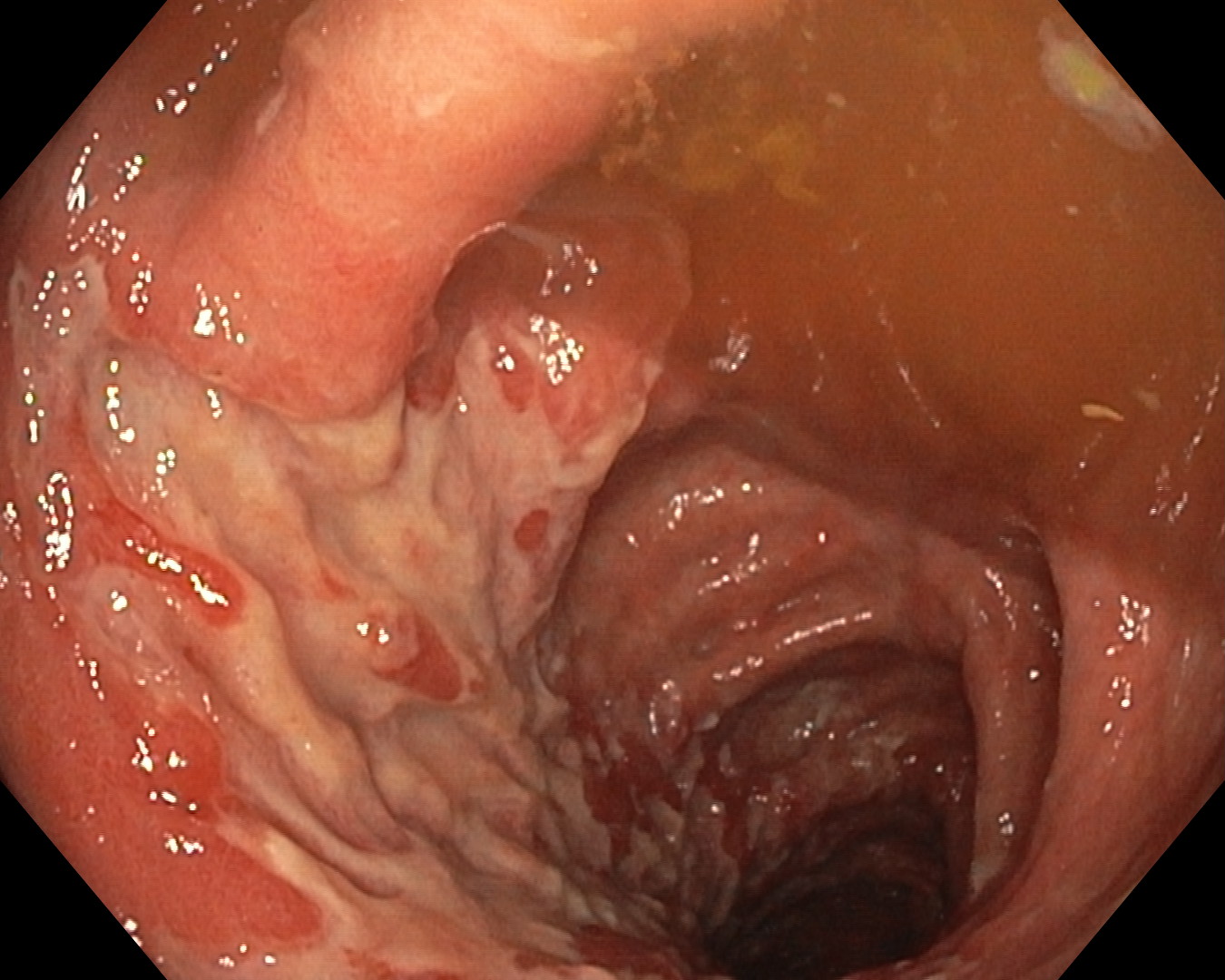
Upper GI endoscopy revealed large esophageal varices with red markings on the surface and fundic gastric varices with stigmata of recent hemorrhage (Figure 1). 2 ml of Histoacryl were injected in the gastric varices to ensure hemostasis (Film 1).
Diagnostic :
Upper digestive bleeding from gastric varices (GOV2).
Discussion :
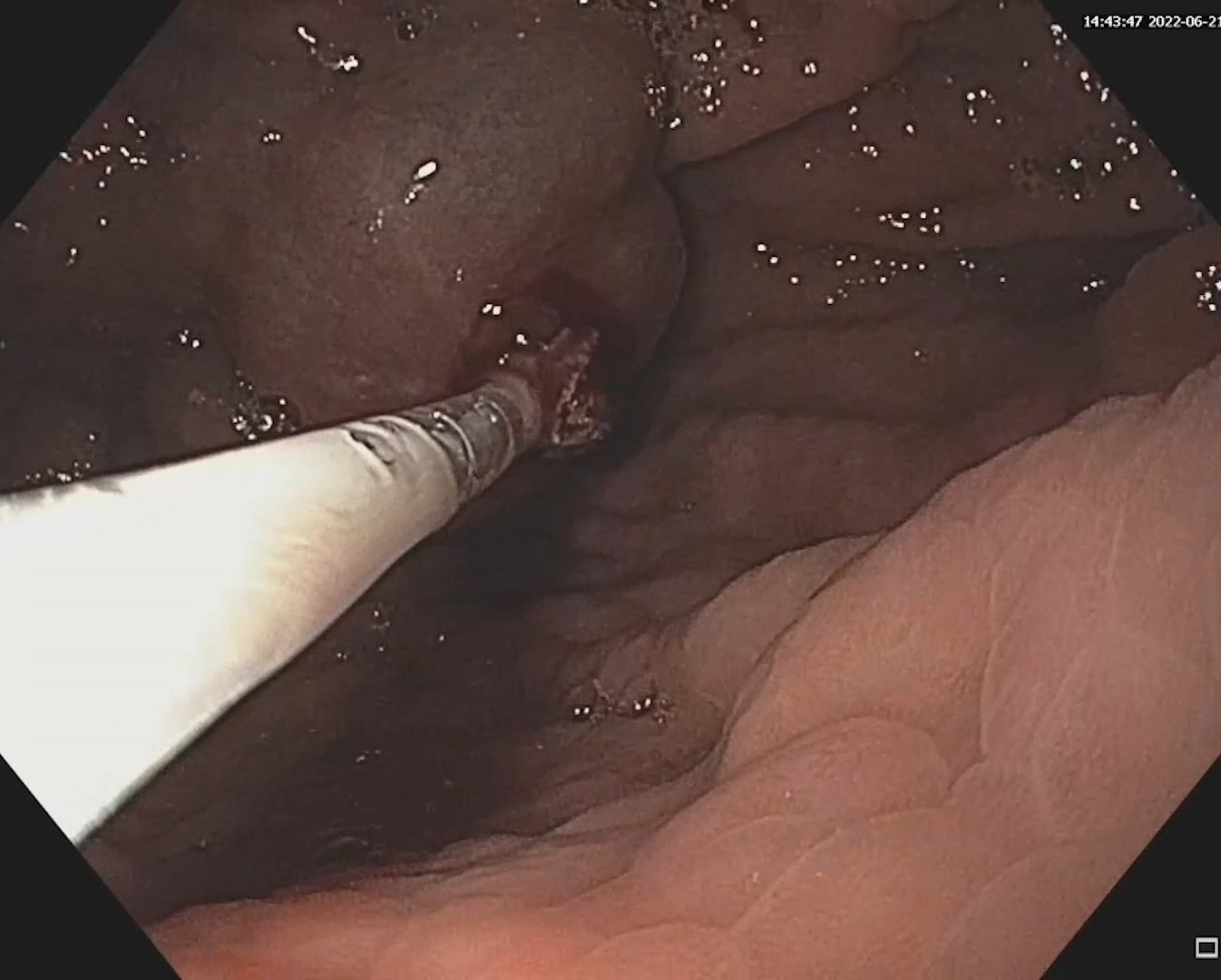
Gastric varices frequently develop in patients with portal vein obstructions. Bleeding occurs less often than esophageal bleeding but is usually severe, associated with increased mortality. The method of choice for obtaining hemostasis is injection of tissue adhesives (Histoacryl) intravariceally. The adhesive rapidly polymerizes in contact with blood and causes vascular occlusion (Figure 2). After the injection, the endoscope is removed with the non-retracted catheter, which is cut externally so as not to damage the biopsy channel (Figure 3). Complications of this technique are rare but potentially severe: pulmonary embolism/stroke and infections. Placing elastic ligatures to varices located in the fornix is usually difficult, especially when they are bulky, and is associated with an increased risk of rebleeding, so it is not usually recommended. Endoscopically guided injection, in combination of cyanoacrylate and coils, seems to bring advantages.
Conclusion :
Injection of cyanoacrylate (Histoacryl) is the treatment of choice for gastric varices.
References :
1. Henry Z, Patel K, Patton H, Saad W. AGA Clinical Practice Update on Management of Bleeding Gastric Varices: Expert Review. Clin Gastroenterol Hepatol 2021; 19: 1098-1107.
2. Philips CA, Ahamed R, Rajesh S, George T, Mohanan M, Augustine P. Beyond the scope and the glue: update on evaluation and management of gastric varices. BMC Gastroenterol 2020; 20: 361.
3. Vine LJ, Subhani M, Acevedo JG. Update on management of gastric varices. World J Hepatol 2019; 11: 250-260.