See other cases
EUS-guided gallbladder drainage with LAMS
History :
A 60-year-old man with a history of coronary disease presents with intense abdominal pain in the right upper quadrant associated with marked weight loss, symptoms that started 3 months prior.
Clinical & biological :
Clinical – tender abdomen with guarding, and painful palpatory mass in the right quadrant.
Biological: mild leukocytosis (13630/µL) with neutrophilia (10840/µL), cholestasis syndrome (ALP 228U/L, GGT 119 U/L), inflammatory syndrome (fibrinogen 433 mg/dL, CRP 24.20mg/L) and increased values of tumor marker CA 19-9 (>1000U/mL).
Imaging :
Abdominal ultrasound revealed multiple hypoechoic nodular lesions distributed in both liver lobes and a distended gallbladder with a large amount of sludge, thickened walls and pericholecystic edema, and an image suggestive of a parietal abscess at the level of the cholecystic fundus.
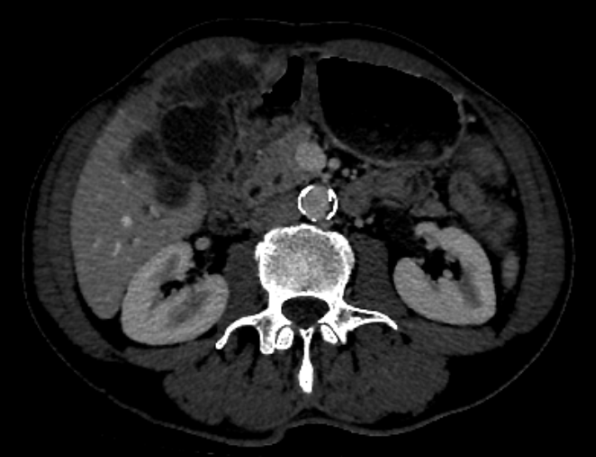
Thoraco-abdominal-pelvic contrast enhanced computed-tomography described acute cholecystitis with multiple adjacent liver abscesses (Figure 1), thickening of the infundibulum and neck region, with multiple infracentimetric lesions and satellite adenopathies, having a CT appearance suggestive for an infundibular gallbladder tumor with liver and lymph nodes metastases.
Diagnostic :
Endoscopic ultrasound (EUS) with a 22G fine needle aspiration (Boston, Scientific) was performed from a hilar lymph node and from a nodular liver lesion suggestive for metastasis. The histopathological result revealed infiltration from an adenocarcinoma-type tumor of biliary origin.
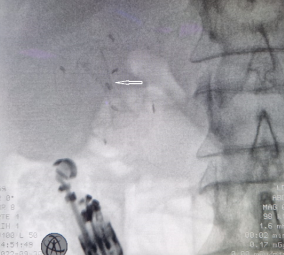
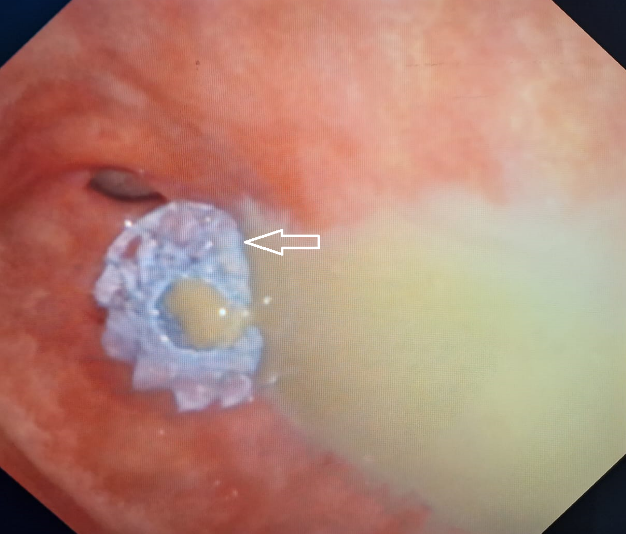
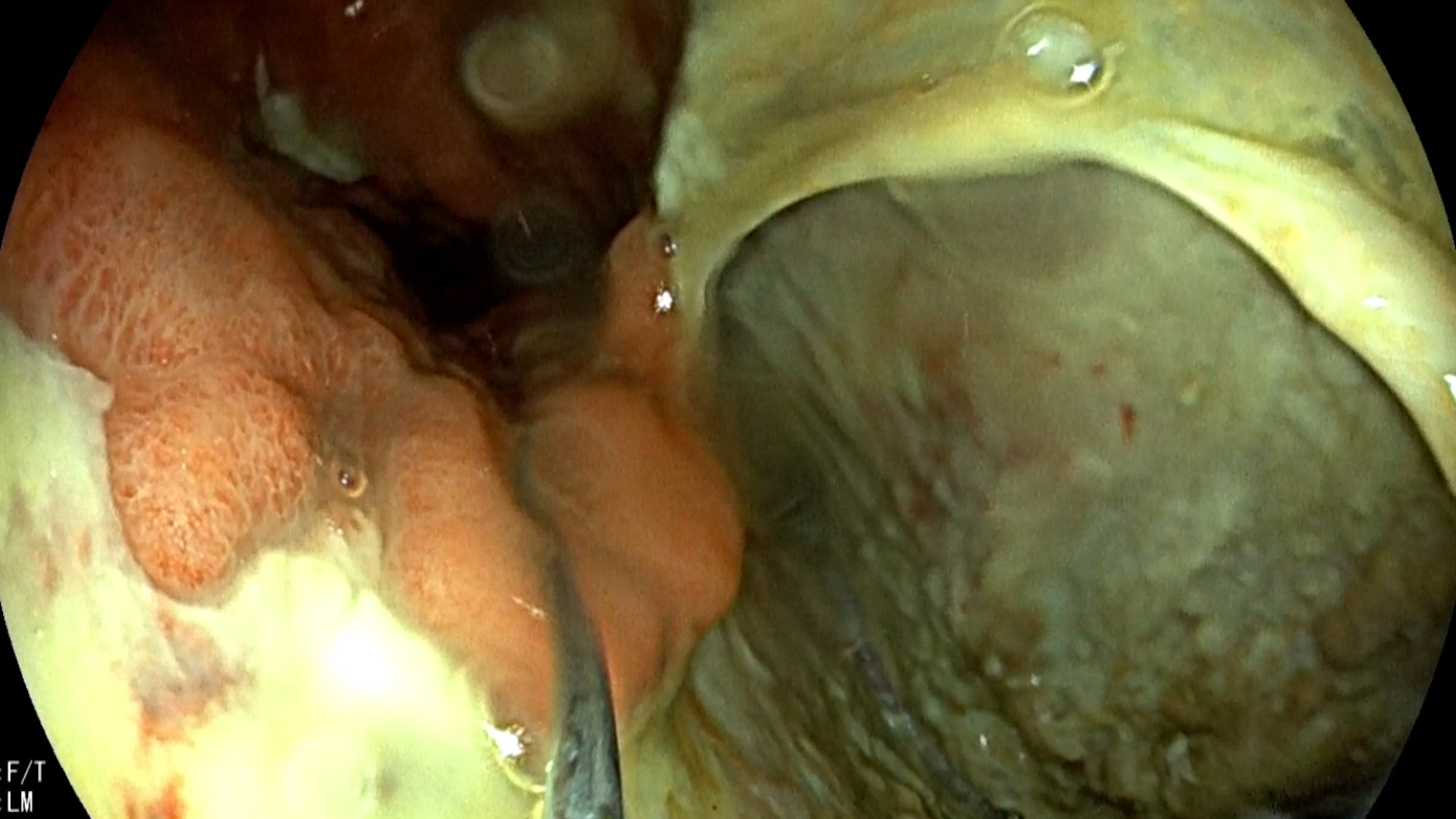
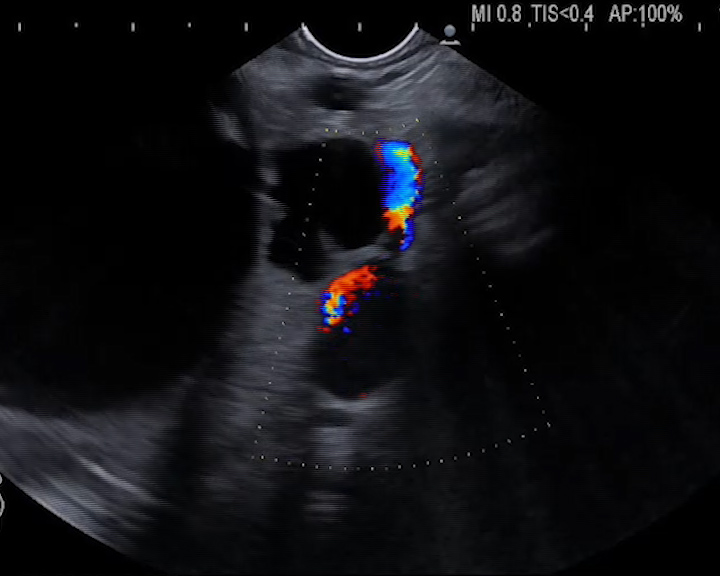
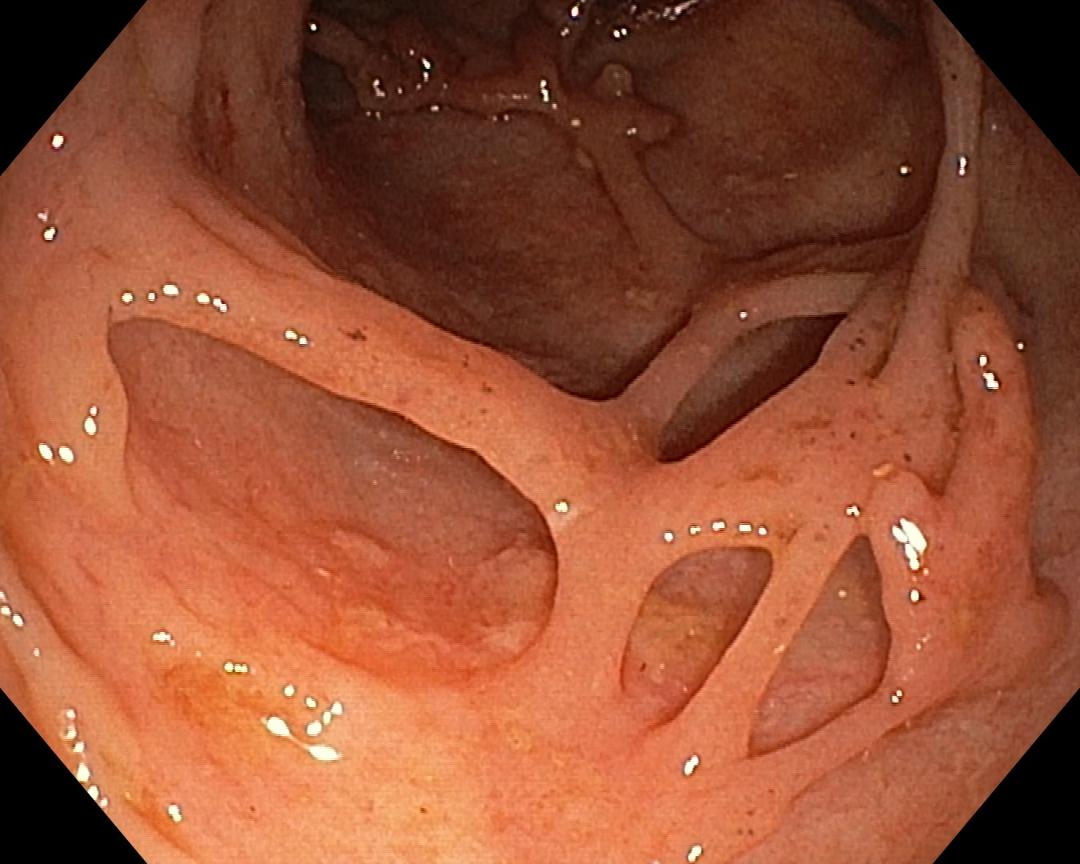
Considering the presence of cholecystitis with associated liver abscesses, the obstruction at the level of the neck of gallbladder, as well as advanced cancer, a minimally invasive approach was decided. EUS puncture of the gallbladder from the stomach was performed with a 19G FNA needle and a guidewire was left in place. Under fluoroscopic and EUS guidance, guidewire aided gallbladder drainage using a lumen apposing metal stent electrocautery enhanced 16/20mm (HotSpaxus, Taewoong) was performed (Figure 2 a, b, c).
After complete evacuation of purulent content into the stomach and large spectrum intravenous antibiotic therapy patient was discharged with good clinical status and chemotherapy treatment was initiated.
Discussion :
Surgical intervention is the gold standard treatment of acute cholecystitis, but it may be contraindicated in patients with multiple comorbidities1. In patients unfit for surgery, the percutaneous transhepatic or endoscopic gallbladder drainage is an alternative.
Percutaneous drainage cannot be performed in the presence of coagulopathy or ascites. In approximately 12% of cases, it is associated with post-procedural pain, and presents the risk of obstruction or displacement of the drain tube, which is why multiple post-procedural interventions are generally required.2
EUS drainage is a new technique, which involves the creation of a fistula between gallbladder and digestive tract (stomach or duodenum). The lumen apposing metal stent (LAMS) has two anchored flanges perpendicular to the lumen of the stent, which allows it to be better fixed to the walls and is completely covered to prevent leakage. Its use for gallbladder drainage has been reported with a success rate of 95.2%.3
Conclusion :
The particularity of this case is represented by the minimally invasive management of acute cholecystitis by placing a transgastric stent, in a patient with multiple comorbidities. The lack of an external drain tube, as well as the possibility of drainage also in the case of patients with ascites, makes this procedure preferable in the case of patients with cholecystitis, in whom surgical intervention is contraindicated.
References :
- Garden OJ, Bradbury AW, Forsythe JLR. Principles and practice of surgery. 4th ed. Edinburgh: Churchill Livingstone; 2002.
- Itoi T, Sofuni A, Itokawa F, et al. Endoscopic transpapillary gallbladder drainage in patients with acute cholecystitis in whom percutaneous transhepatic approach is contraindicated or anatomically impossible (with video) Gastrointest Endosc. 2008;68:455–460.
- Jain D, Bhandari BS, Agrawal N, Singhal S. Endoscopic Ultrasound-Guided Gallbladder Drainage Using a Lumen-Apposing Metal Stent for Acute Cholecystitis: A Systematic Review. Clin Endosc. 2018 Sep;51(5):450-462.