See other cases
Endoscopic Stenting of a Significant Esophageal Perforation After Achalasia Treatment: When Dilation Goes Too Far
History :
A 73-year-old female patient with a known history of achalasia, arterial hypertension, type 2 diabetes mellitus, obesity, and mild dyslipidemia was emergently transferred from another hospital unit. The referral was necessitated by an iatrogenic esophageal perforation sustained during an attempted balloon dilatation procedure.
Immediately following the perforation, an attempt was made to close the defect using hemostatic clips; however, this was unsuccessful due to the extensive size of the perforation. Prior to transfer, the patient received supportive care, including broad-spectrum antibiotics and fluid resuscitation.
Clinical & biological :
- Clinical examination: The patient presented in a moderately altered general condition. She was conscious, cooperative, and hemodynamically stable. A mild fever of 37.3°C was noted. The patient reported retrosternal chest pain and an inability to swallow (dysphagia).
- Laboratory findings: Laboratory investigations revealed mild systemic inflammation, with leukocytosis (11,500/μL) and neutrophilia (9,200/μL). C-reactive protein (CRP) was markedly elevated at 250 mg/L. Liver function tests showed elevated transaminases, with both alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels approximately eight times the upper limit of normal, indicative of hepatic cytolysis.
Imaging :
Combined Endoscopic and Surgical Management
Following preoperative optimization with fluid resuscitation and antibiotic prophylaxis, a multidisciplinary team comprising gastroenterologists and surgeons proceeded with a hybrid endoscopic-surgical intervention under general anesthesia with orotracheal intubation. The procedure consisted of two main stages:
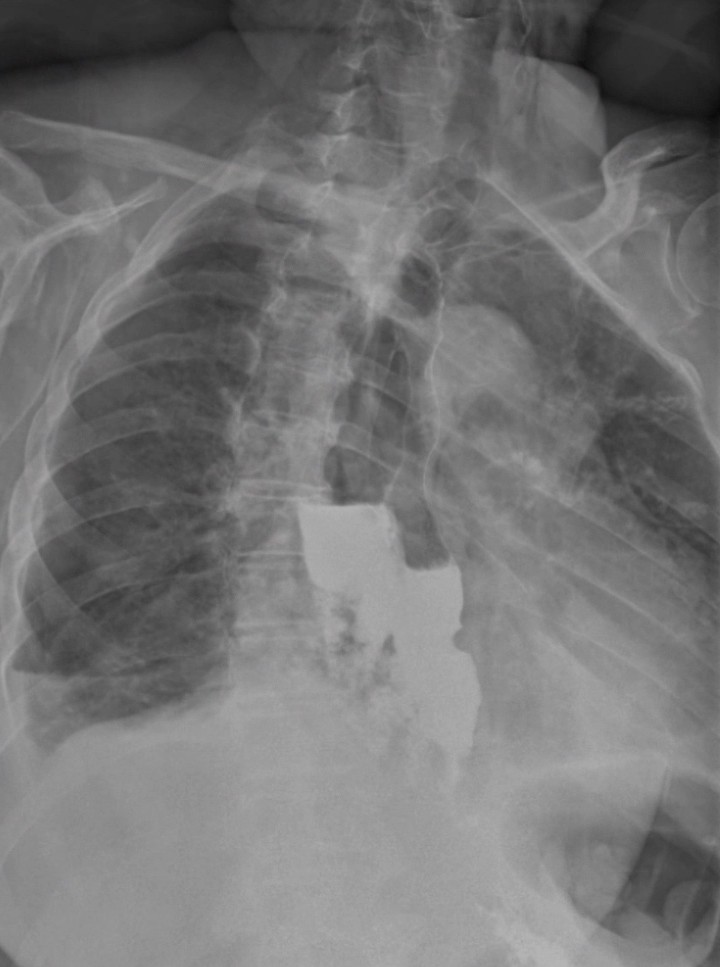
- Endoscopic intervention: Endoscopy revealed a large esophageal perforation extending from 25 cm to 34 cm from the dental arch ( 1-2). The lower esophageal sphincter, located at 37 cm, exhibited marked spasticity and was traversed with significant difficulty. The gastric mucosa appeared normal. A metallic guidewire was introduced into the first portion of the duodenum, and under endoscopic guidance, a fully covered self-expandable metallic stent (155 mm in length, 23 mm in diameter) was deployed across the perforation site. The stent was secured distally using four hemostatic clips (Fig. 3).
- Surgical intervention: A thoracoscopic approach was used to evacuate approximately 150–200 mL of hemorrhagic pleural fluid, followed by debridement of necrotic tissue and placement of thoracic drainage. During the laparoscopic phase, dissection of the diaphragmatic crura allowed access to the thoracic cavity. The esophageal perforation was further debrided, and a drainage tube was positioned through the esophageal hiatus adjacent to the fistulous tract. Additionally, a surgical jejunostomy was established for enteral nutrition.
Post-Procedural Evolution and Imaging
The patient’s immediate postoperative course was favorable, with improvement in her general condition and minimal drainage output. However, a contrast esophagogram performed on postoperative day two revealed no passage of contrast into the stomach, due to persistent lower esophageal sphincter spasm related to her underlying achalasia. Instead, the contrast material was diverted into the space between the stent and the esophageal wall, with subsequent extravasation into the mediastinum via the fistulous tract.
Following multidisciplinary team consultation, a decision was made to place a second stent within the existing stent to facilitate passage through the gastroesophageal junction, restore physiologic flow into the stomach, and eliminate further leakage through the perforation site.
Second Endoscopic Procedure
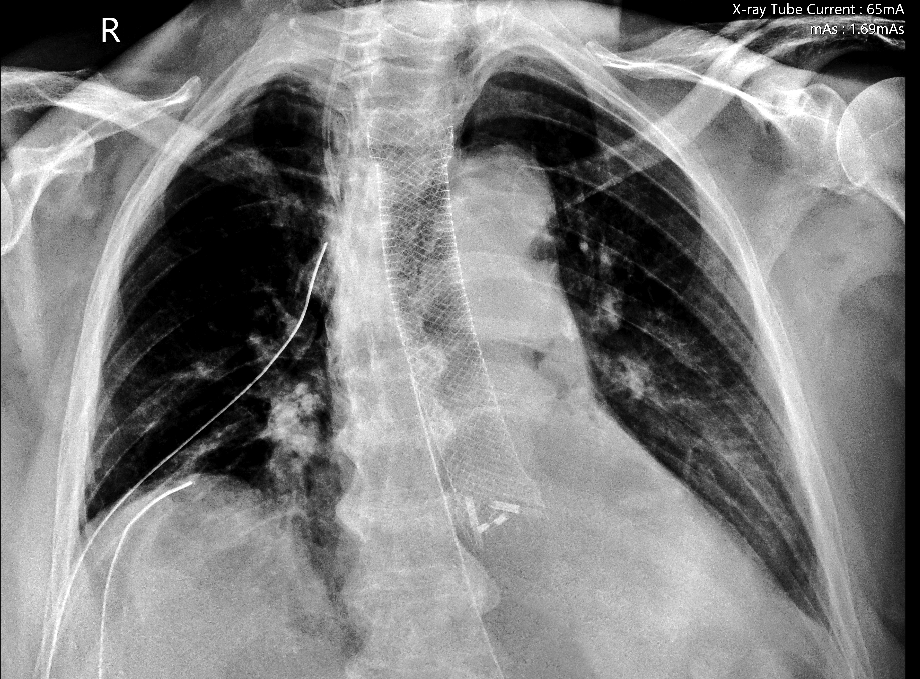
During the second endoscopic procedure, the initially placed stent was found to be in proper position. After overcoming the challenge of navigating the spastic lower esophageal sphincter, a Savary guidewire was advanced into the second portion of the duodenum. Using combined endoscopic and fluoroscopic guidance, a second fully covered self-expandable metallic stent (155 mm x 23 mm) was deployed coaxially within the first stent. The proximal end was positioned at 30 cm, and the distal end extended into the gastric lumen (Fig. 4).
Imaging
A computed tomography (CT) scan performed after the second intervention confirmed the correct placement of both metallic stents. There was no evidence of contrast extravasation during oral contrast administration, indicating satisfactory containment of the esophageal contents.
Clinical Outcome
The patient demonstrated progressive clinical improvement throughout her hospital stay. Drain output remained minimal, and systemic parameters normalized. After two weeks of hospitalization, she was discharged with instructions to maintain exclusive oral hydration and nutrition.
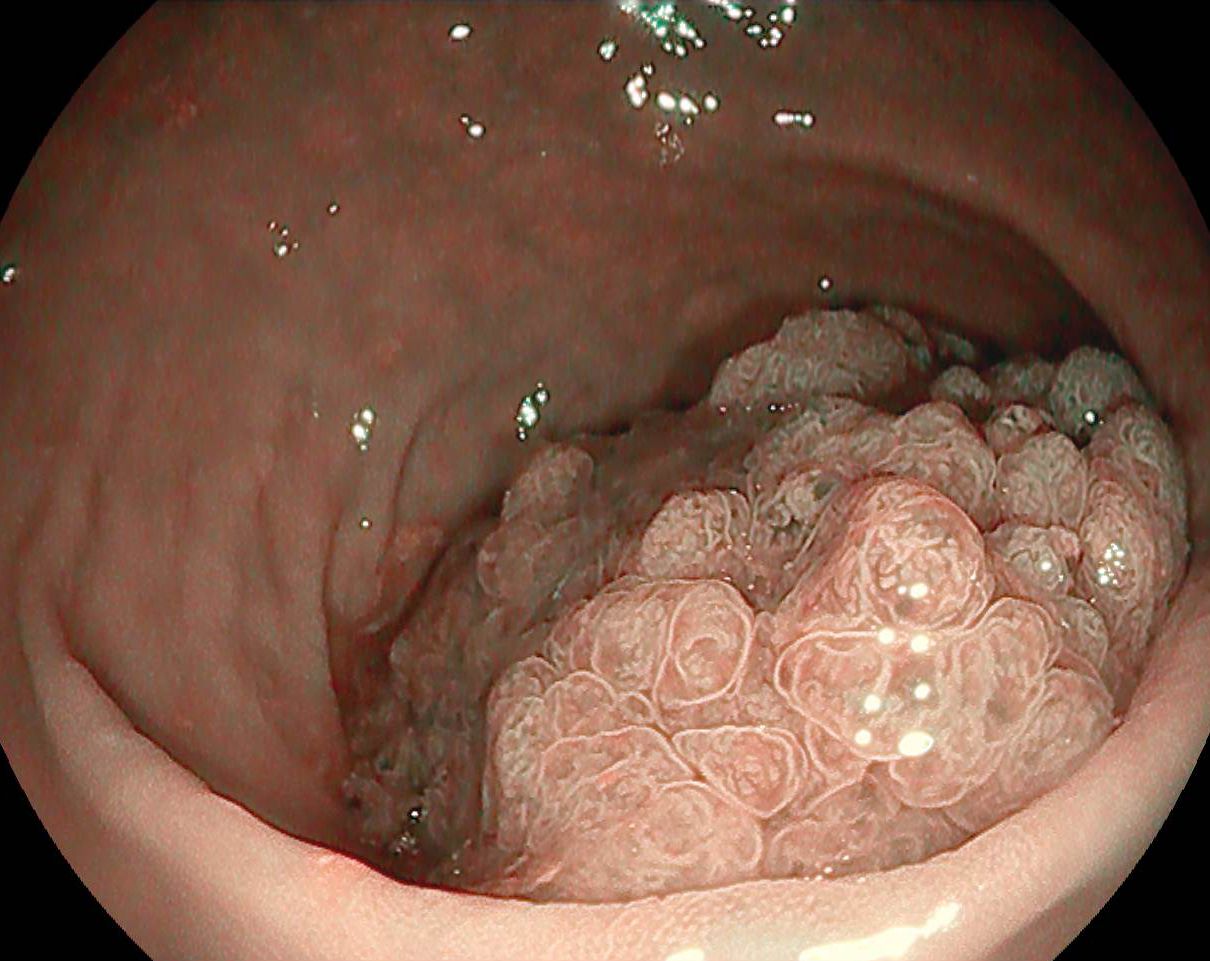
The stents remained in situ for four weeks. Following elective endoscopic removal, the esophageal mucosa showed complete regeneration, and the perforation was entirely healed (Fig. 5-7). There was an apparent small persistent fistula but the follow-up contrast esophagogram confirmed the absence of any residual communication.
Diagnostic :
Esophageal double stenting for a complex perforation induced by pneumatic balloon dilation for achalasia.
Discussion :
Fully covered self-expandable metallic stents (SEMS) represent an effective therapeutic modality for the management of esophageal perforations and fistulas. By isolating the perforation site from intraluminal contents, these stents create an optimal environment for tissue regeneration and healing. The fully covered design prevents ingrowth and reduces the risk of stent migration or leakage through the stent interstices (1).
While small esophageal perforations may be successfully managed using hemostatic clips or a single metallic stent, larger defects—such as in the present case—require a more complex, multidisciplinary approach. This includes collaboration between gastroenterologists, surgeons, radiologists, and nutrition specialists (2,3).
A notable particularity in this case was the presence of untreated achalasia, leading to a hypertonic lower esophageal sphincter. This contributed to functional obstruction and stasis, exacerbating the mediastinal leakage. The decision to place a second stent within the first was crucial in restoring luminal patency and preventing further extraluminal contamination.
Conclusion :
Although, fully covered SEMS represent an effective therapeutic modality for the management of esophageal perforations and fistulas, larger defects—such as in the present case—require a more complex, multidisciplinary approach.
References :
- Ong GKB, Freeman RK. Endoscopic management of esophageal leaks. J Thorac Dis. 2017 Mar;9(Suppl 2):S135-S145. doi: 10.21037/jtd.2017.03.100. PMID: 28446977; PMCID: PMC5384896.
- John A, Chowdhury SD, Kurien RT, David D, Dutta AK, Simon EG, Abraham V, Joseph AJ, Samarasam I. Self-expanding metal stent in esophageal perforations and anastomotic leaks. Indian J Gastroenterol. 2020 Oct;39(5):445-449. doi: 10.1007/s12664-020-01078-z. Epub 2020 Oct 1. PMID: 33001339.
- Chiu CH, Leow OQY, Wang YC, Chen WH, Fang HY, Chao YK, Lin J. Esophageal stenting with minimally-invasive surgical intervention for delayed spontaneous esophageal perforation. J Thorac Dis 2023;15(3):1228-1235. doi: 10.21037/jtd-22-1316