See other cases
Duodenal submucosal tumor
History :
A 55-year-old patient known to have persistent atrial fibrillation receiving anticoagulant treatment (Eliquis) with melena was evaluated for upper gastrointestinal bleeding.
Clinical & biological :
Clinical: pallor.
Paraclinical: acute post-hemorrhagic anemia (hemoglobin = 10 g/dL).
Imaging :
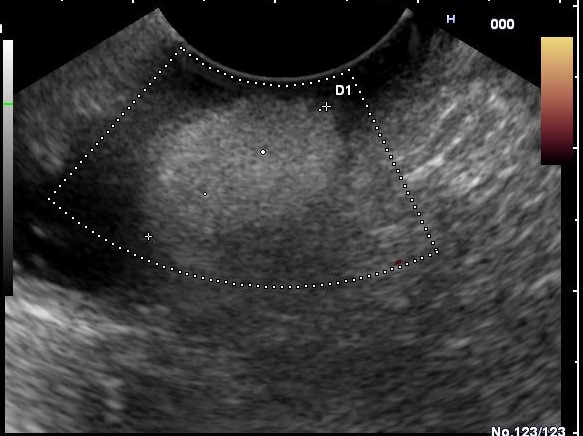
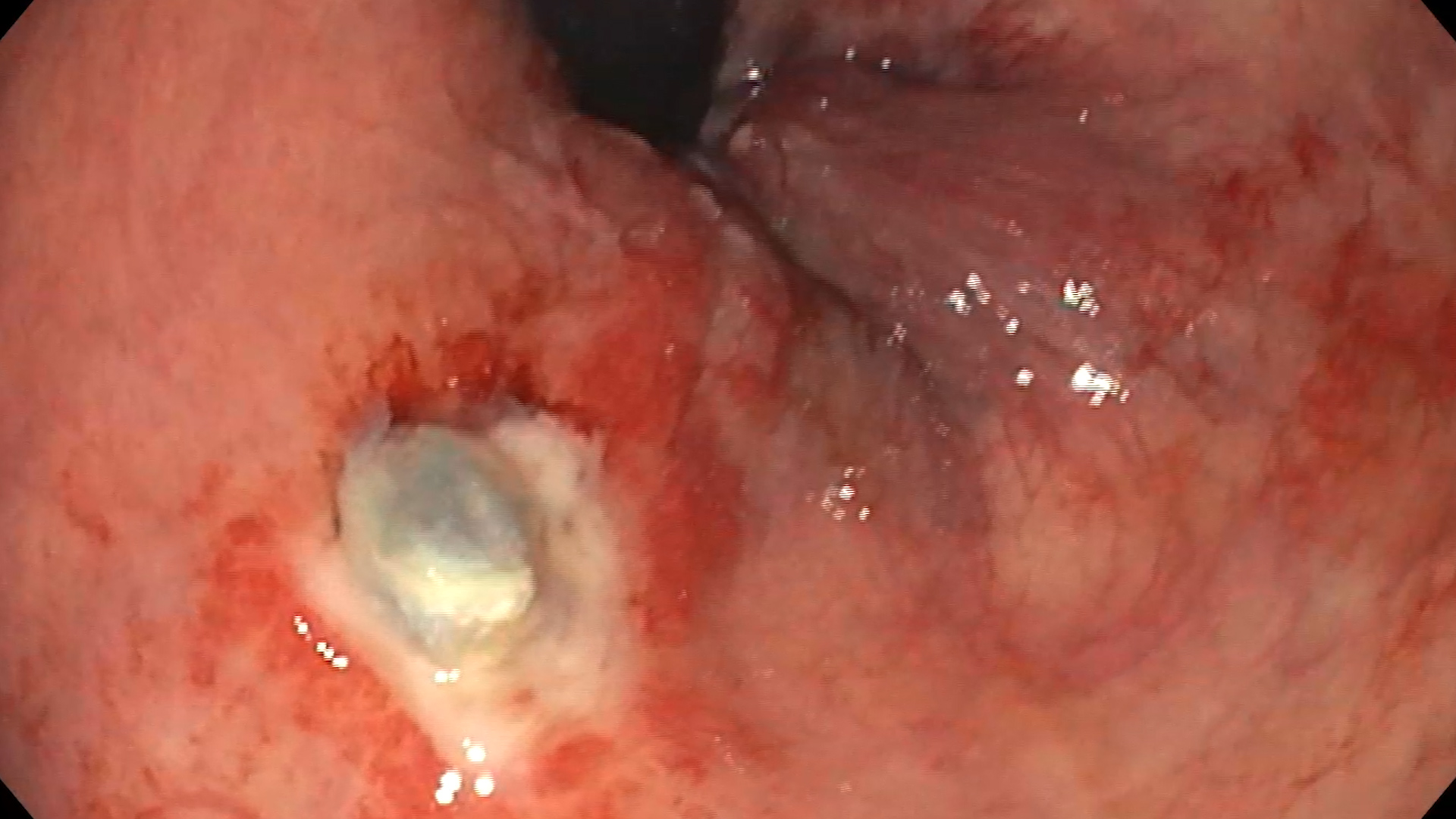
Upper GI Endoscopy showed a pedicled polyp of approx. 15 x 10 mm diameter, with normal covering mucosa, both in white light (Figure 01), and i-SCAN mode (Figure 02). Endoscopic ultrasound indicated a hyperechoic mass, with absent Power Doppler signal, located in the third layer (submucosa) (Figure 03).
Diagnostic :
What treatment option are you considering?
1. Endoscopic follow-up
2. Cold snare polpectomy
3. Endo-Loop placement and endoscopic resection with polypectomy loop
4. Injection of diluted epinephrine (1:10 000) and endoscopic resection with polypectomy loop
5. Surgery
Discussion :
Digestive lipomas are rare benign submucosal formations, generally asymptomatic, but which can cause digestive bleeding or other complications related to their large size (obstruction, invagination). The endoscopic appearance is usually characteristic, with a normal-looking mucosa, sometimes slightly yellowish. Ecoendoscopically, lipomas are visualized as hyperechoic formations, located in the 3rd layer (submucosa), with absent Doppler signal, except for the pedicle where vessels may be present.
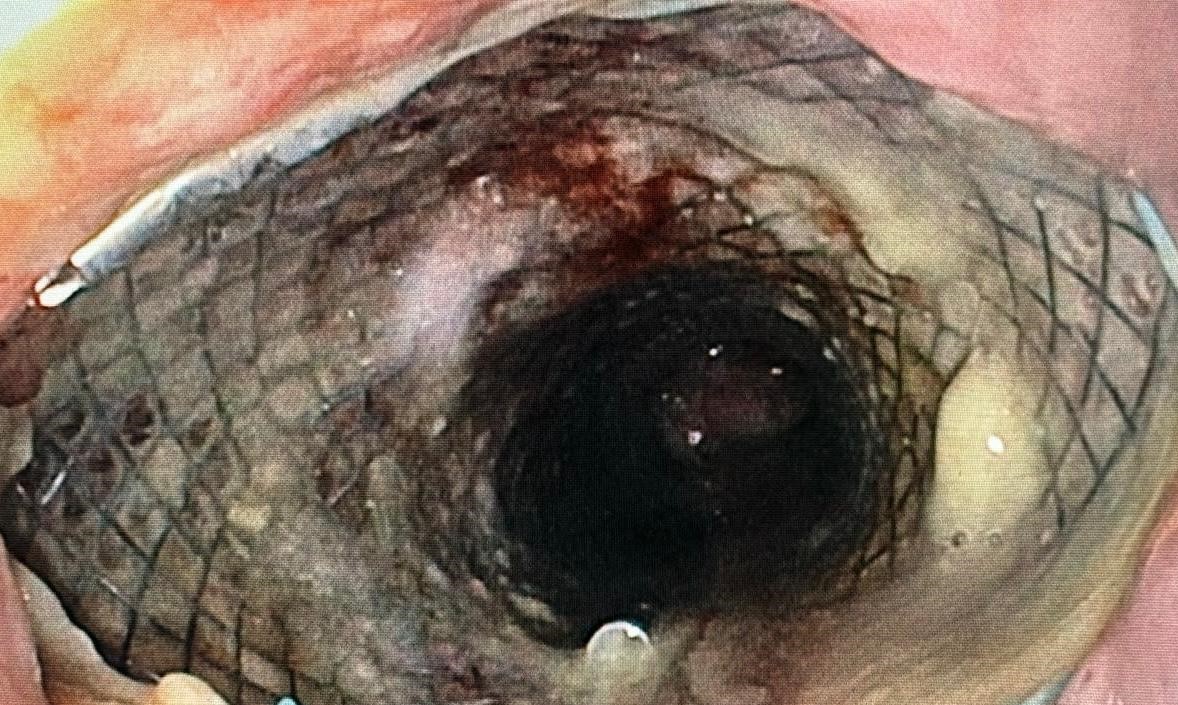
Endoscopic resection is a useful technique as an alternative to surgery, although experience is limited to some case reports. Due to the risk of major complications (perforation / bleeding), most authors prefer to place a nylon band (EndoLoop) at the base of the pedicle, followed by loop polypectomy. Other authors prefer placement of metal clips at the base and then loop resection. Endoscopic resection should always be weighed against the benefits and risks.
Conclusion :
Duodenal lipomas are rare conditions that can cause diagnostic and management difficulties.
References :
1. Sou S, Nomura H, Takaki Y, Nagahama T, Matsubara F, Matsui T, Yao T. Hemorrhagic duodenal lipoma managed by endoscopic resection. J Gastroenterol Hepatol. 2006; 21(2): 479-81.
2. Murata A, Osoegawa T, Ijyu M, Kanayama K, Tanaka M, Nakamura K. Pedunculated duodenal lipoma treated with endoscopic polypectomy with a detachable snare. Fukuoka Igaku Zasshi. 2008; 99(6): 131-5.
3. Lee SH, Park JH, Park DH, Chung IK, Kim HS, Park SH, Kim SJ, Cho HD. Endoloop ligation of large pedunculated submucosal tumors (with videos). Gastrointest Endosc 2008; 67(3): 556-60.
4. Aydin HN, Bertin P, Singh K, Arregui M. Safe techniques for endoscopic resection of gastrointestinal lipomas. Surg Laparosc Endosc Percutan Tech 2011; 21(4) :218-22.