See other cases
Duodenal OTSC
History :
A 70 year old male was admitted for vomiting and diarrhea, symptoms started 24h before presenting to the hospital. No abdominal pain, no fever/chills. Recent medical history shows atrial fibrillation and prothrombin mutation with multiple episodes of pulmonary embolism (Acenocumarol treatment; chronic heart failure; hypertension; pulmonary hypertension; right knee prosthesis with multiple surgical interventions including an episode of sepsis – chronic antibiotic treatment at home (Amoxicillin + Tetracycline); mild cognitive disorder.
Clinical & biological :
Patient is alert and partially oriented. Cardiorespiratory stable. No abdominal pain, no abdominal masses detected. Normal stool on rectal digital exam. Nasogastric tube inserted in the emergency department shows no fresh or digested blood present.
Slight inflammation (leukocytosis and elevated CRP), acute kidney injury; INR 8.3 (patient on Acenocumarol at home); Rapid Clostridoides difficile stool test is positive; normal hemoglobin levels.
Imaging :
No active lesions on head CT scan;
Cardiology consult suggests Enoxaparin during hospital stay, switch to Apixaban at home due to lower bleeding rates;
Infectious diseases suggests starting oral Vancomycin and stopping oral antibiotics (Amoxicillin and Tetracycline).
Endoscopy performed on the 7th day after admission (hematemesis in large quantities):
- Grade D esophagitis, antral gastritis and duodenitis; large blood clot spanning from the distal stomach up to the descending duodenum. Large Forrest Ia ulcer localized in the duodenal bulb. Successful hemostasis achieved with injection therapy and thermal forceps.
Repeated endoscopy on 12th and 16th days after admission (steady drop in serum hemoglobin and melena present):
- Normal mucosa seen in esophagus, stomach and duodenum, same duodenal ulcer now Forrest Ib, injection and thermal therapy achieves hemostasis.
Repeated endoscopy on 21st day after admission (planning discharge)
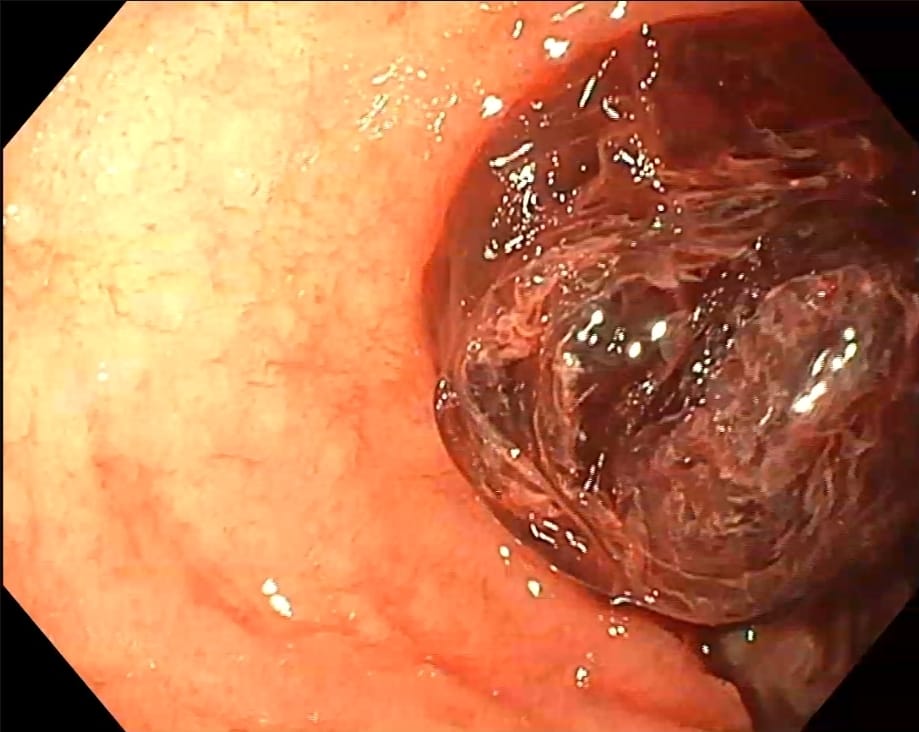
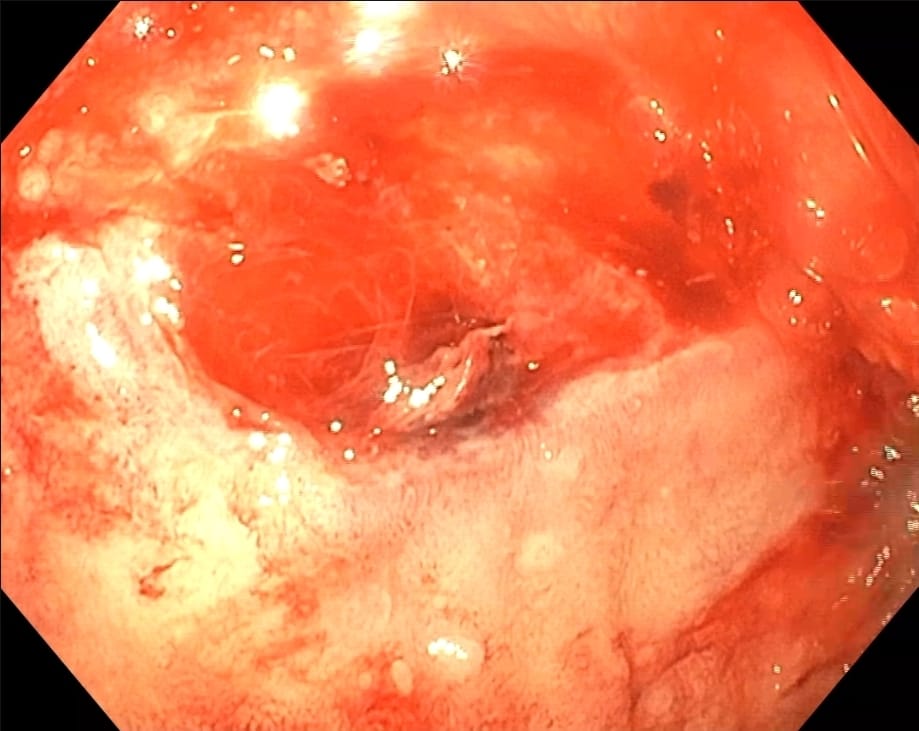
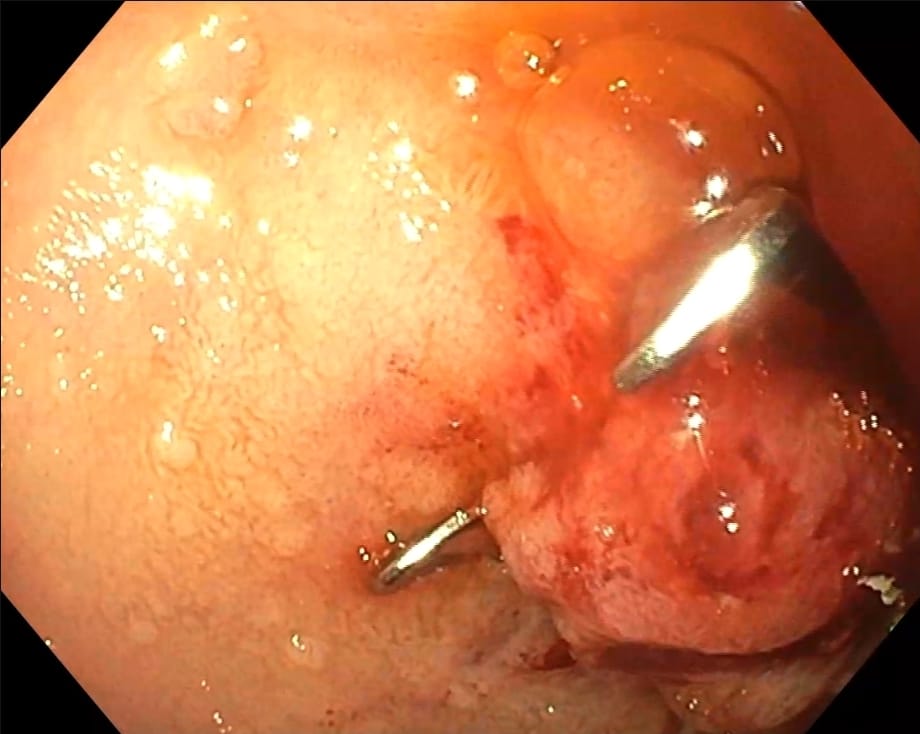
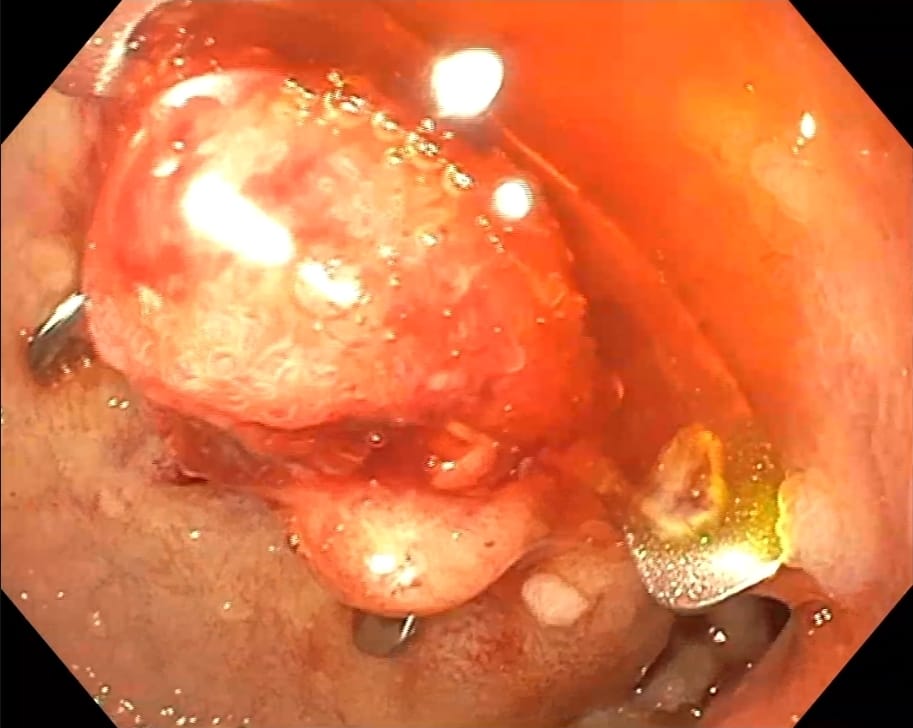
- Large blood clot (Photo 1) adherent to duodenal ulcer (Photo 2), 30mm in size, Forrest 2a, injection therapy with subsequent over the scope clip (OVESCO) achieves hemostasis (Photo 3,4; Film 1).
Diagnostic :
Large duodenal ulcer with persistent bleeding in spite of first line endoscopic therapies.
Severe esophagitis, gastritis and duodenitis.
Clostridioides difficile infection in patient needing high dose PPI therapy.
Thrombophilia needing chronic anticoagulation.
Discussion :
Endoscopic hemostasis can be achieved using injection, thermal, and/or mechanical modalities, and it has been well demonstrated that any endoscopic hemostasis therapy is superior to pharmacotherapy alone in patients with FIa, Fib and FIIa ulcers.
ESGE (2021) [1] recommends for patients with actively bleeding ulcers (FIa, FIb), combination therapy using epinephrine injection plus a second hemostasis modality (contact thermal or mechanical therapy). In selected actively bleeding ulcers (FIa, FIb), specifically those > 2 cm in size, with a large visible vessel > 2mm, or located in a high risk vascular area (e. g., gastroduodenal, left gastric arteries), or in excavated/fibrotic ulcers, endoscopic hemostasis using a cap-mounted clip should be considered as first-line therapy. Ulcers with “persistent bleeding” (bleeding refractory to standard hemostasis) should benefit from cap mounted clips or hemostatic spray/powder.
As this was not a simple case of a peptic ulcer, definitive endoscopic hemostasis was needed in order to discharge the patient, high doses of PPI therapy could not be administered due to active Clostridoides infection (with recurrence very likely due to chronic antibiotic treatment) and the patient needs long term anticoagulation (switched to Apixaban from Acenocumarol for lower bleeding rates) due to a history of pulmonary embolisms due to prothrombin mutation and atrial fibrilation.
Definitive long term hemostasis was achieved with an over-the-scope-clip (OVESCO) as it not only remains attached to the mucosa for a long period (multiple weeks), it grips a much larger area compared to the standard through-the-scope clips.
Multiple studies have been done since ESGE published its guidelines in 2021 that discuss over-the-scope-clips as first line therapy for upper or lower gastro-intestinal bleeding instead of the usual thermal/mechanical therapy with or without injection therapy [2,3].
Conclusion :
Using over-the-scope-clips might be a better solution as first-line therapy in a multitude of cases where standard first-line therapy might fail due to patient related factors, even if standard therapy might seem adequate judging by the lesion aspect alone.
References :
- Gralnek IM, Stanley AJ, Morris AJ, et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2021. Endoscopy. 2021;53(3):300-332. doi:10.1055/a-1369-5274
- Richter-Schrag HJ, Glatz T, Walker C, Fischer A, Thimme R. First-line endoscopic treatment with over-the-scope clips significantly improves the primary failure and rebleeding rates in high-risk gastrointestinal bleeding: A single-center experience with 100 cases. World J Gastroenterol. 2016;22(41):9162-9171. doi:10.3748/wjg.v22.i41.9162
- Richter-Schrag HJ, Glatz T, Walker C, Fischer A, Thimme R. First-line endoscopic treatment with over-the-scope clips significantly improves the primary failure and rebleeding rates in high-risk gastrointestinal bleeding: A single-center experience with 100 cases. World J Gastroenterol. 2016;22(41):9162-9171. doi:10.3748/wjg.v22.i41.9162