See other cases
Drain or pain? The art of unclogging malignant biliary obstructions
History :
A 79-year-old female patient, with a history of operated and radiotreated breast cancer, presents with sclero-cutaneous jaundice and pruritus.
Clinical & biological :
The patient was conscious, cooperative, underweight, complains of insomnia, presents with sclero-cutaneous jaundice and pruritus, dark urine, and acholic stools.
Imaging :
CT: Suggests a pancreatic head tumor and reveals intra- and extrahepatic bile duct dilation with multiple metastatic liver lesions.
MR: Findings indicative of a proliferative process in the pancreatico-duodenal groove, biliary obstruction in the preampullary region, marked intra- and extrahepatic bile duct dilations, and secondary hepatic lesions.
Diagnostic :
ERCP attempt: Initial bile duct cannulation attempt fails with a 0.035-inch guidewire, followed by another failure with a 0.025-inch guidewire; the procedure was abandoned.
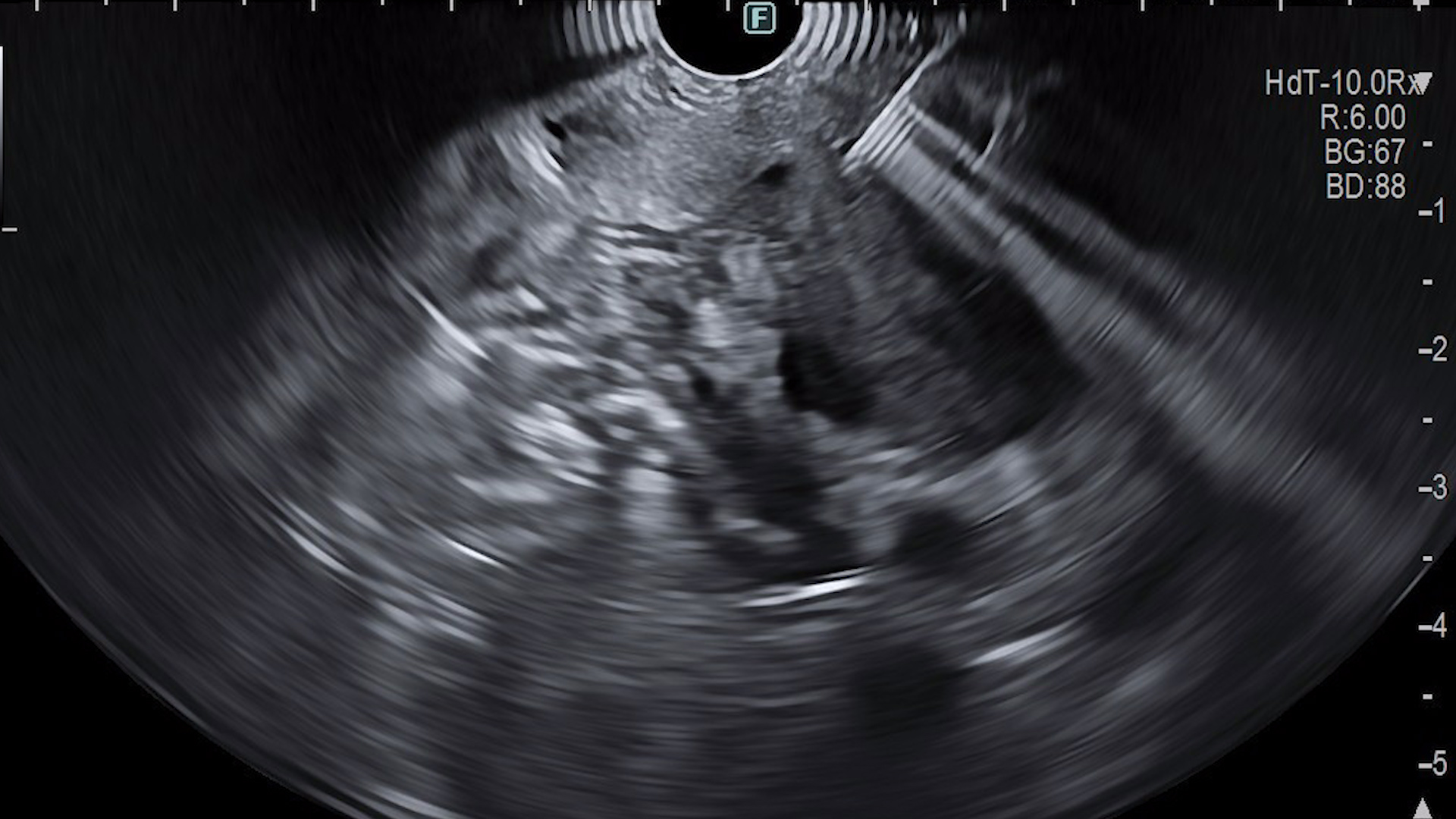
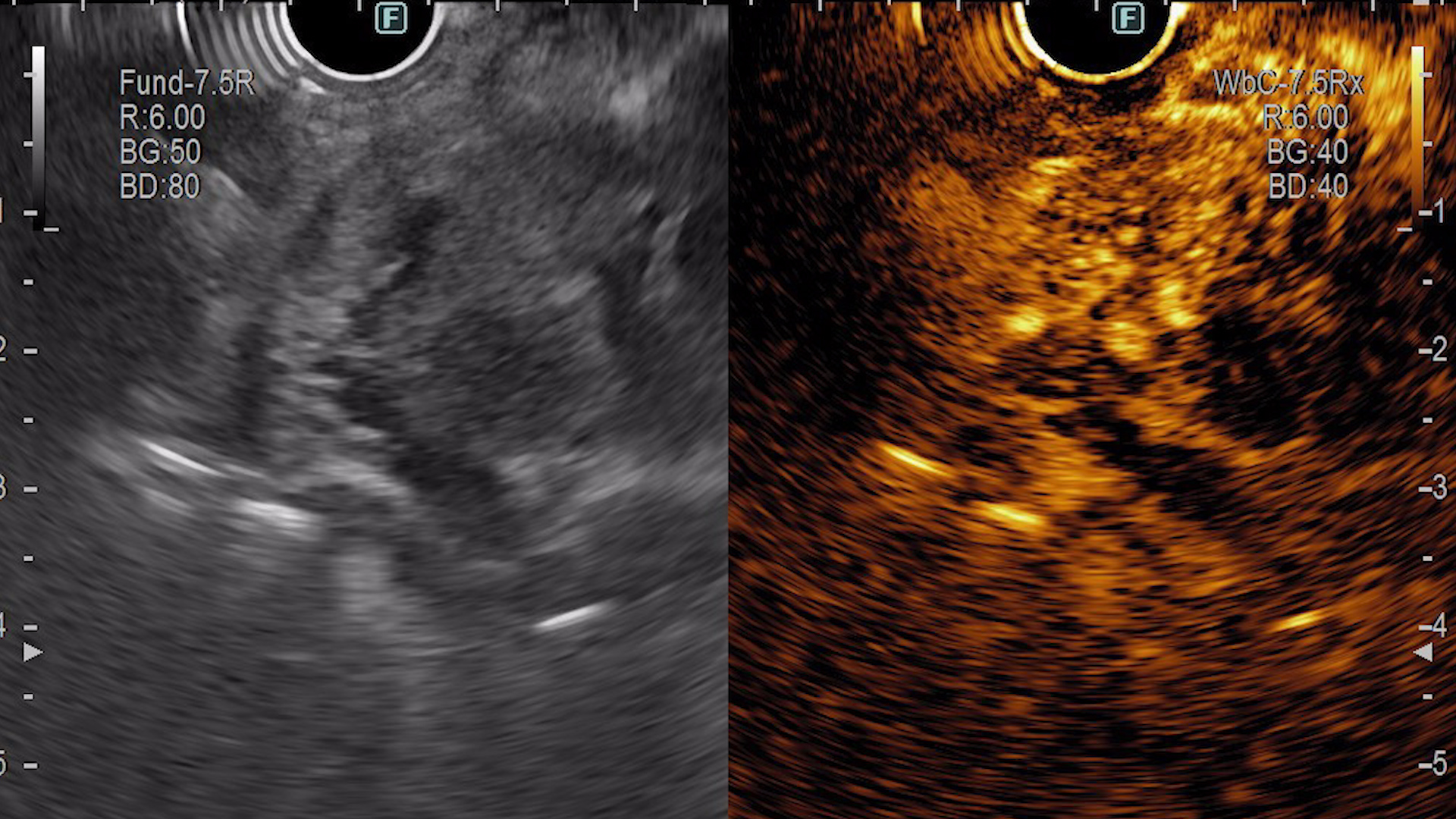
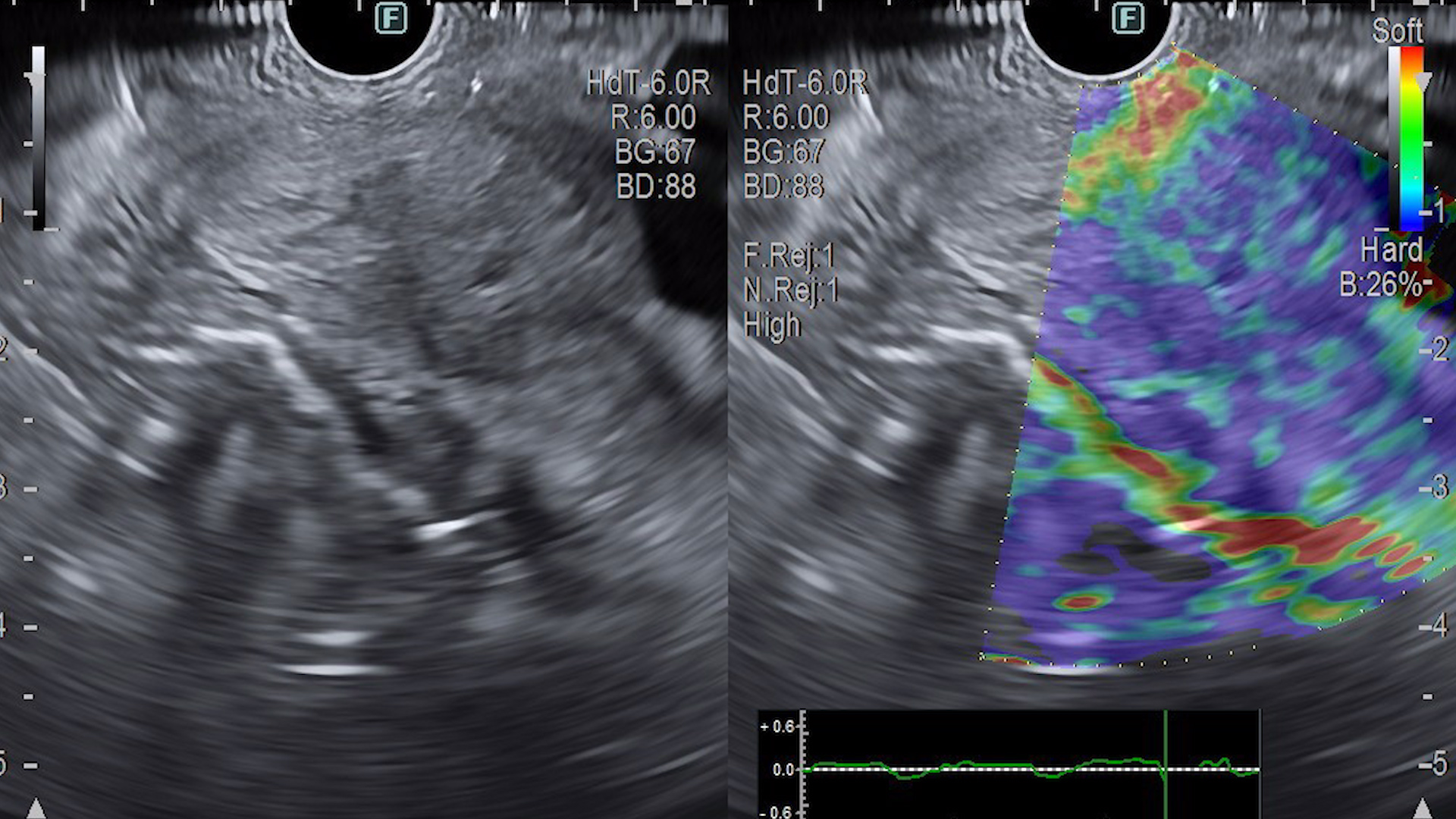
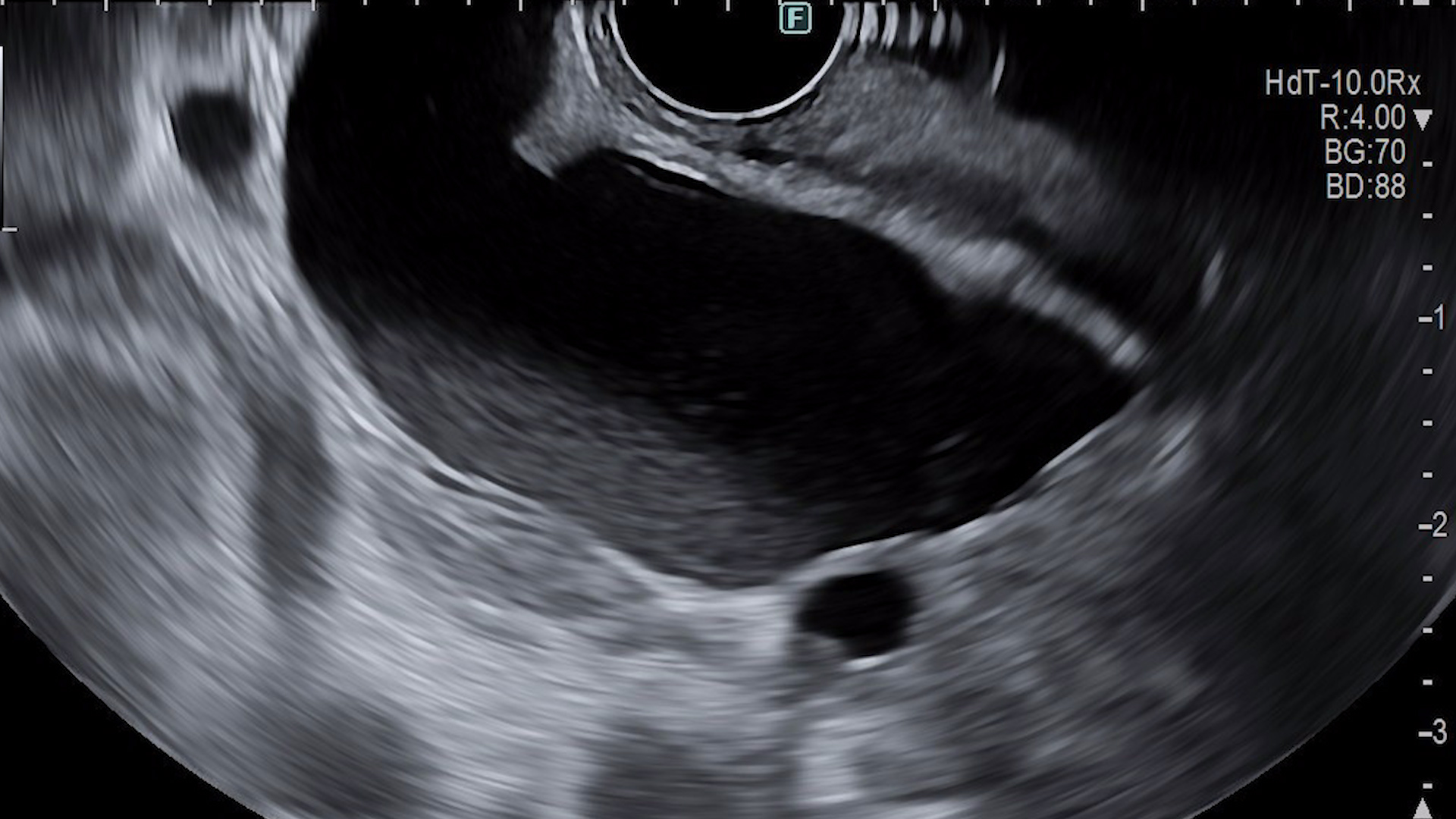
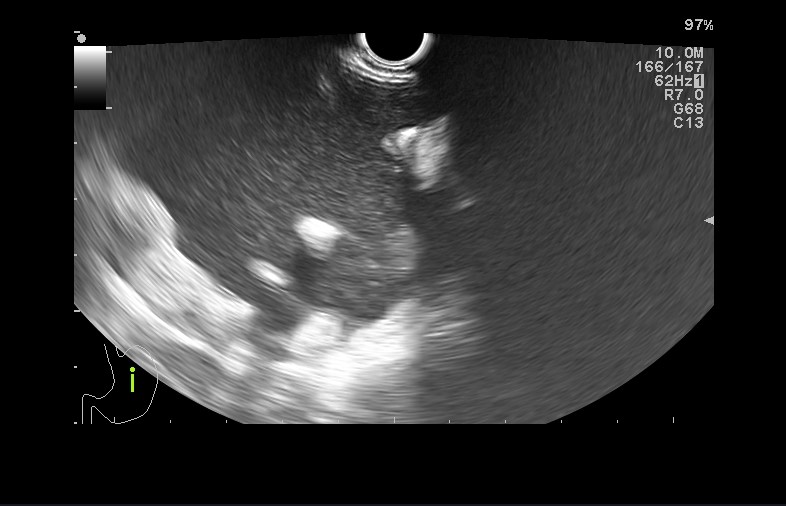
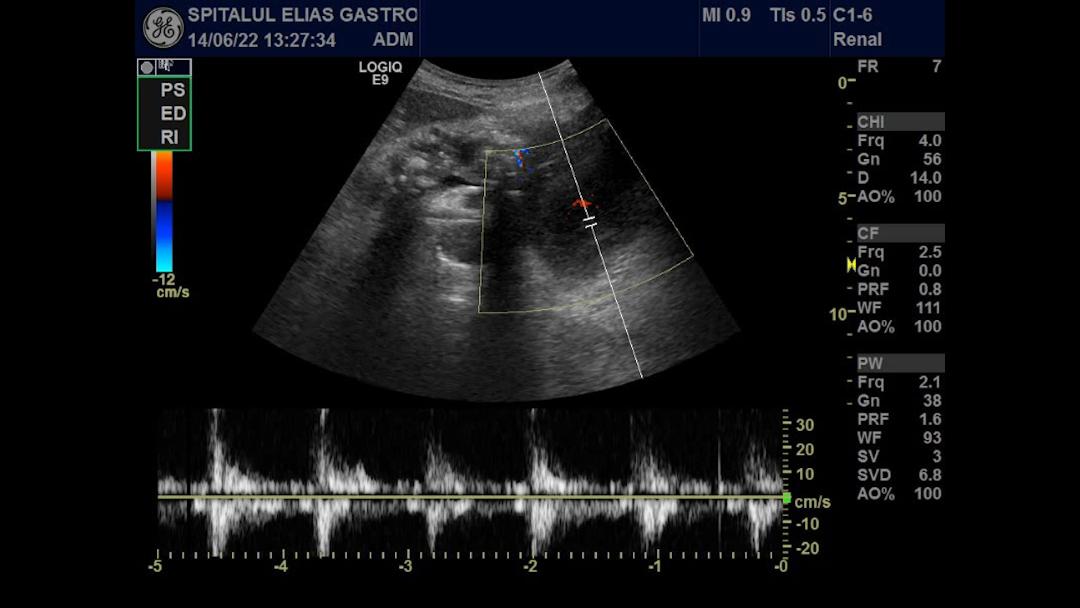
Diagnostic endoscopic ultrasound: Fine-needle biopsy of the tumor in the papillary projection area, involving the common bile duct and pancreatic duct (Figure 2-4). Confirmation of secondary hepatic lesions.
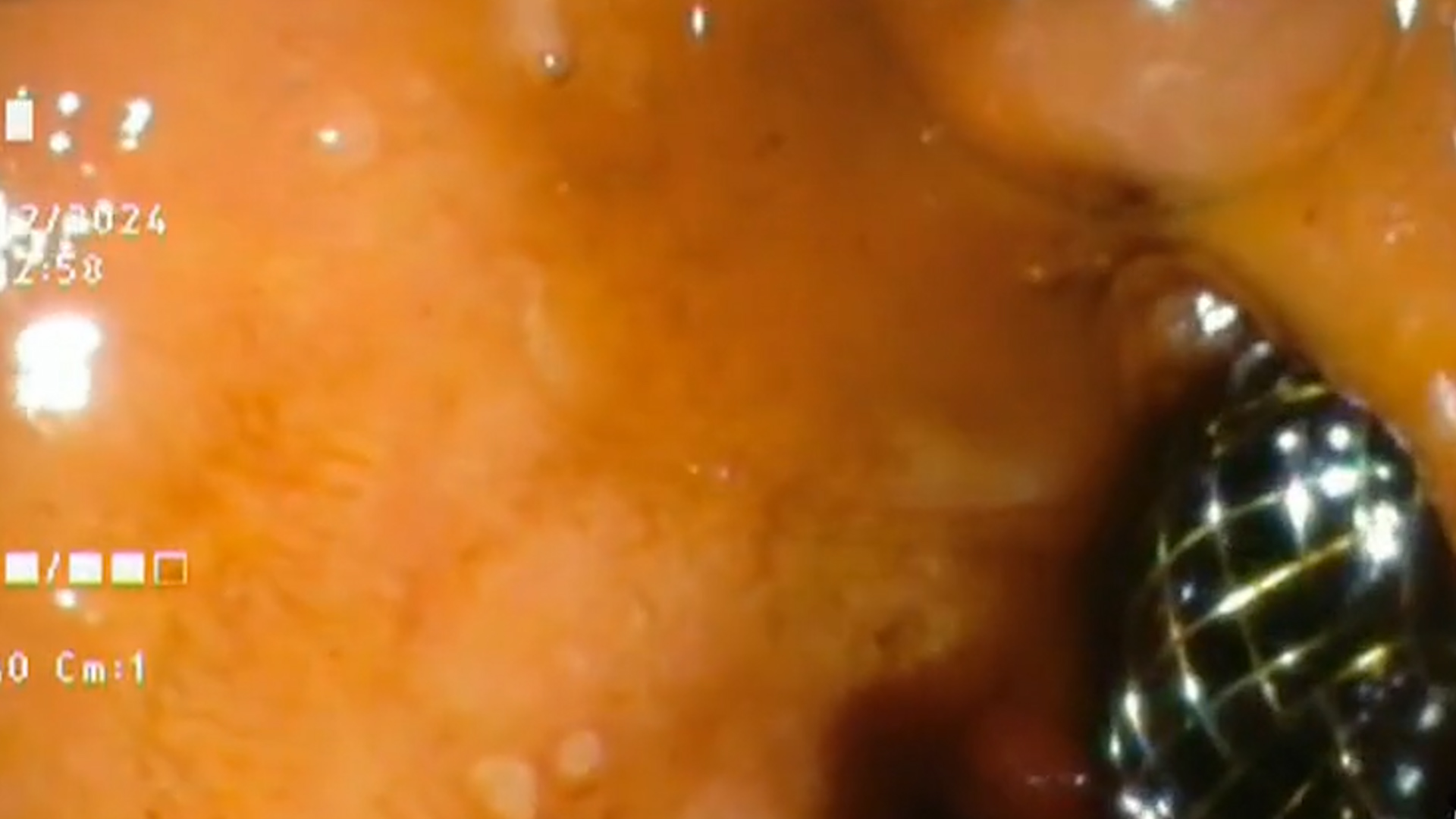
Therapeutic endoscopic ultrasound: EUS-guided bile duct drainage (choledochoduodenostomy) with a Hotaxios 8/8 mm stent and collection of bile cultures, which tested positive for Enterococcus (Figura 5-7).
Histopathological Diagnosis: Histological appearance and immunohistochemical profile consistent with well-differentiated adenocarcinoma (G1).
Discussion :
Malignant distal biliary obstruction is most commonly caused by pancreatic cancer, cholangiocarcinoma, or metastases. In this case, imaging investigations identified an ampullary mass, with EUS-BD being considered a better alternative than PTBD, when ERCP fails, allowing both biliary drainage and tissue sampling. Compared to ERCP, EUS-guided choledochoduodenostomy (EUS-CDS) offers a similar success rate.
For benign tumors, EUS-guided rendez vous (EUS-RV) is preferred.
For malignant tumors, when there is access to the duodenal papilla:
- Proximal biliary obstructions: EUS-HGS or EUS-RV is preferred.
- Distal biliary obstructions: EUS-CDS, EUS-HGS, or EUS-RV is preferred.
If papilla access is obstructed:
- Proximal biliary obstructions: EUS-HGS is preferred.
- Distal biliary obstructions: EUS-CDS or EUS-HGS is preferred.
Stent misdeployment, relatively common in EUS-CDS, is associated with an extrahepatic bile duct diameter of ≤ 15 mm and can be avoided by deploying hallway the distal flange while the catheter is pushed more distally.
Conclusion :
EUS-BD is an effective alternative to PTBD, after ERCP failure, as it allows both biliary drainage and tissue sampling, making it the preferred method in certain cases.
References :
- Chen YI, Sahai A, Donatelli G, Lam E, Forbes N, Mosko J, et al. Endoscopic Ultrasound-Guided Biliary Drainage of First Intent With a Lumen-Apposing Metal Stent vs Endoscopic Retrograde Cholangiopancreatography in Malignant Distal Biliary Obstruction: A Multicenter Randomized Controlled Study (ELEMENT Trial). Gastroenterology. 2023 Nov;165(5):1249-1261.e5. doi: 10.1053/j.gastro.2023.07.024. Epub 2023 Aug 6. PMID: 37549753.
- Dietrich CF, Braden B, Burmeister S, Aabakken L, Arciadacono PG, Bhutani MS, et al. How to perform EUS-guided biliary drainage. Endosc Ultrasound 2022;11:342-54. doi: 10.4103/EUS-D-21-00188. PMID: 36255022.
- American Society for Gastrointestinal Endoscopy guideline on the role of therapeutic EUS in the management of biliary tract disorders: summary and recommendations. Gastrointest Endosc. 2024 Dec;100(6):967-979. doi: 10.1016/j.gie.2024.03.027. Epub 2024 Jul 29. PMID: 39078360.
- Khoury T, Sbeit W, Fumex F, Marasco G, Eusebi LH, Fusaroli P, Chan SM, Shahin A, Basheer M, Gincul R, Leblanc S, Teoh AYB, Jacques J, Lisotti A, Napoléon B. Endoscopic ultrasound- versus ERCP-guided primary drainage of inoperable malignant distal biliary obstruction: systematic review and meta-analysis of randomized controlled trials. Endoscopy. 2024 Dec;56(12):955-963. doi: 10.1055/a-2340-0697. Epub 2024 Jun 6. PMID: 38843824.
- Chen YI et al, ELEMENT and DRA-MBO working groups. Stent misdeployment and factors associated with failure in endoscopic ultrasound-guided choledochoduodenostomy: analysis of the combined datasets from two randomized trials. Endoscopy. 2024 Dec 16. doi: 10.1055/a-2463-1601. Epub ahead of print. PMID: 39505002.
- Shah J, Jena A, Jearth V, Singh AK. Modified technique for deployment of a lumen-apposing metal stent during endoscopic ultrasound-guided choledochoduodenostomy in minimally dilated duct. Endoscopy. 2023 Dec;55(S 01):E416-E417. doi: 10.1055/a-2008-0431. Epub 2023 Feb 9. PMID: 36758629; PMCID: PMC9911296.