See other cases
Diminutive hyperplastic polyp
History :
A 55-year-old man who presented for colonoscopic evaluation, performed as part of an opportunistic screening program.
Clinical & biological :
Within normal limits.
Imaging :
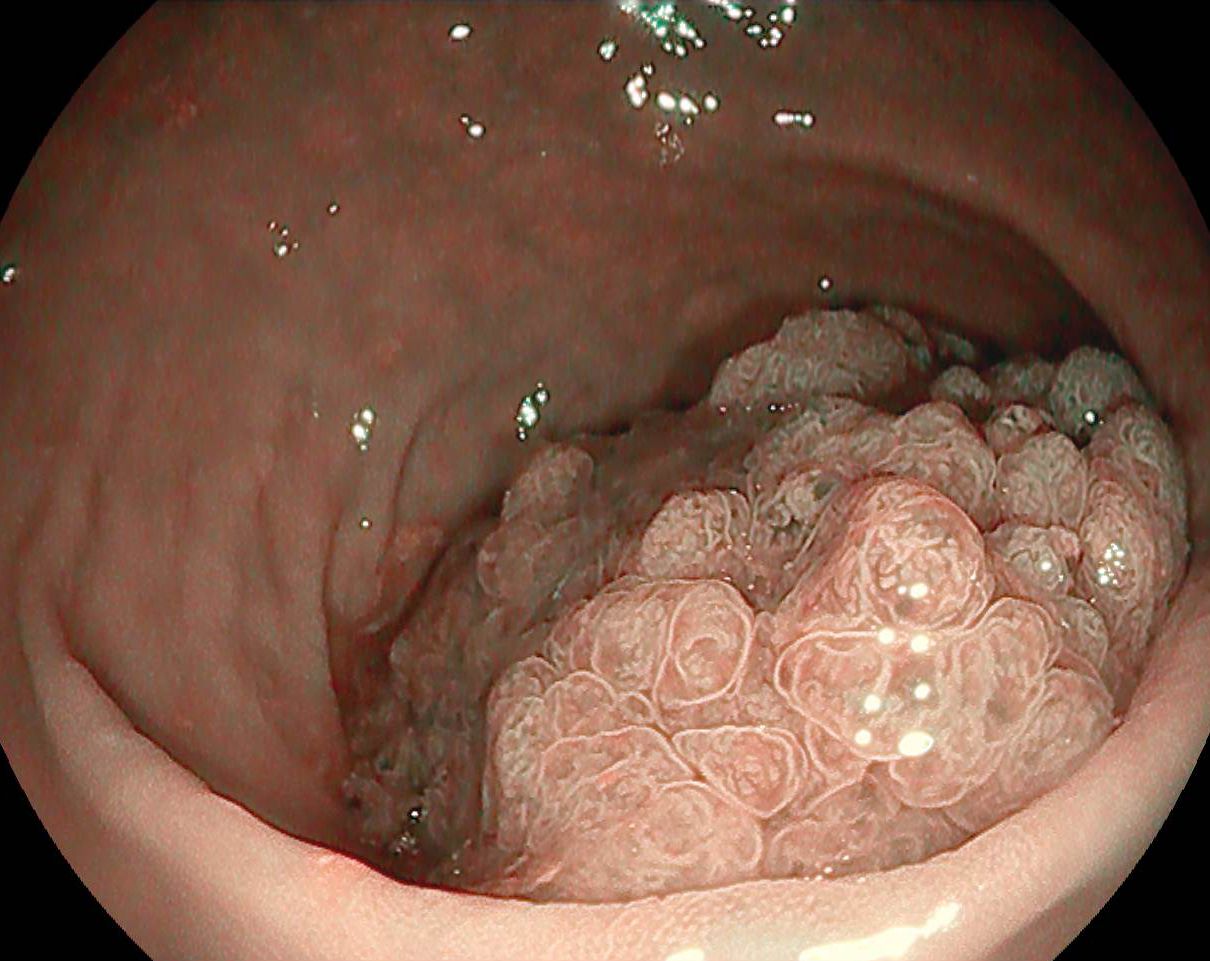
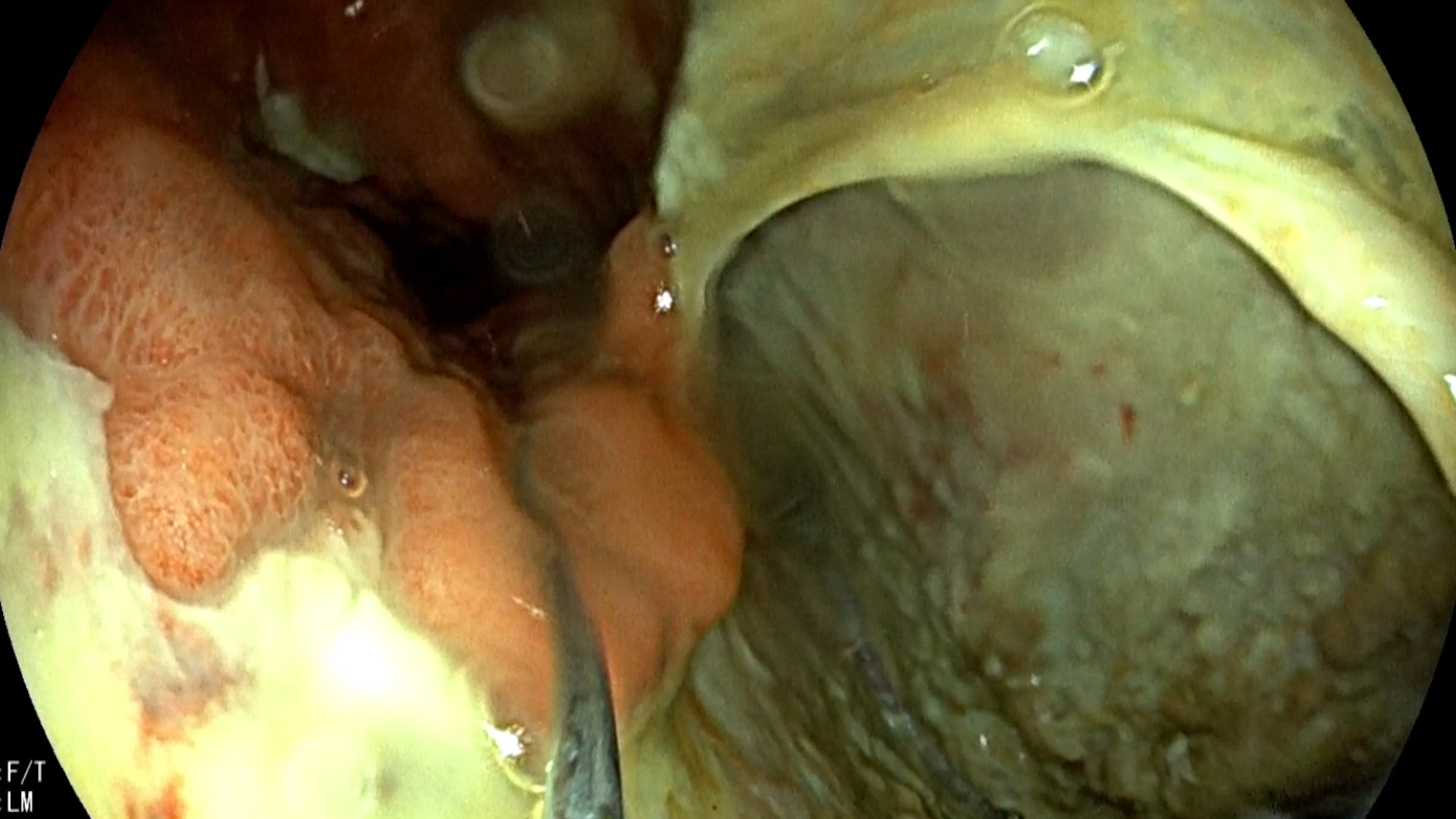
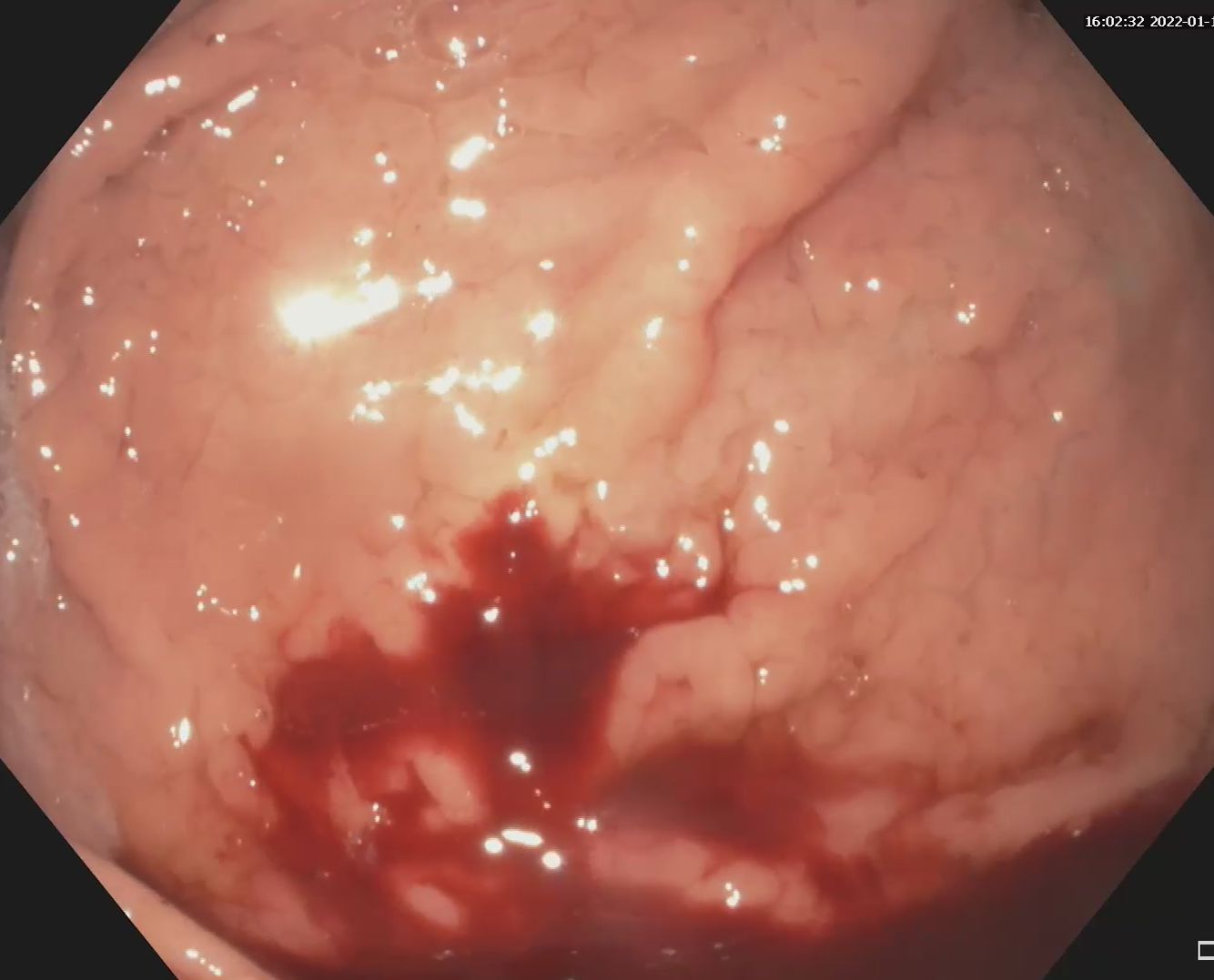
Colonoscopy identified multiple diminutive flat polyps of approx. 3-5 mm, type J-NET 1 (NICE 1), which were resected by cold snare polypectomy (CSP) (Figure 1-3, Movie 1). Polyps were aspirated into the biopsy channel in a polyp trap for histopathological examination. The technique of using a cold snare is different from a hot snare resection. The lesion must be positioned at 5 o’clock, the tip of the catheter a few mm away and the loop must be fully open and placed completely over the lesion. Once placed completely over the polyp, the loop should be closed in a continuous maneuver (“close and cut”) while maintaining pressure on the loop and the colonic wall respectively. Upon closure, the loop will also capture a margin of normal tissue. Insufflation must be maintained, aspiration is not recommended because it can favor submucosa trapping, which can prevent cutting. Immediate bleeding is usually insignificant and, from experience, delayed bleeding does not occur. In the case of cold excision, the entrapped polyp should not be lifted, nor should the loop be closed/opened during the maneuver to preserve the margin of normal tissue and keep the specimen in the loop.
Diagnostic :
Cold snare polypectomy is now the primary technique of choice for resection of polyps up to 10 mm in size because it eliminates the risk of perforation and delayed bleeding, and visual feedback allows real-time assessment of immediate bleeding (1,2). The diagnosis was established based on the histopathological examination which confirmed the presence of hyperplastic polyps.
Discussion :
An unsolved problem with the cold snare technique is how the endoscopist must handle the situation when the snare wire fails to cut the tissue and the snare remains trapped in the wall (probably because it catches too much submucosal tissue). It is possible that repeated opening and/or closing maneuvers compromise the margin of normal tissue, resulting in histologically incomplete resection. The general principles are: (1) minimize deep submucosal entrapment by maintaining insufflation and avoiding aspiration (or perform underwater polypectomy); (2) maintaining full loop closure for up to 10 seconds, as a slow transition may occur; close the loop completely and, if necessary, in a slow and controlled maneuver, partially reopen to release the entrapped submucosa while gently lifting the lesion from the colonic wall. The goal is to open the loop thread just a little – enough to release the excess white band of submucosa, while keeping the loop “under” the lesion. It is important to avoid completely reopening the loop.
If the lesion fails to cut with the cold snare:
– Keep the loop tightly closed for 10-15 seconds.
– Maintain full insufflation and avoid aspiration.
– Make sure the endoscope is straight.
– Angle the tip of the endoscope.
– Straighten and stretch the catheter.
– Partially reopen the loop (about 1/3 of the loop handle; avoid fully opening).
– Slowly lift the lesion off the colon wall.
– Take care to release the trapped submucosa (a white band) under the lesion.
– Lower the lesion (to prevent its loss).
– Close the loop completely again to cut the lesion.
– It is not known whether it is safe or effective to apply electrocautery to a lesion that has failed to cut with the cold loop.
Conclusion :
Cold snare polypectomy (CSP) is considered the technique of choice for resection of diminutive and small (below 10 mm) polyps.
References :
1. Shinozaki S, Kobayashi Y, Hayashi Y, et al. Efficacy and safety of cold versus hot snare polypectomy for resecting small colorectal polyps: Systematic review and meta-analysis. Dig Endosc 2018; 30: 592-599.
2. Ferlitsch M, Moss A, Hassan C, et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017; 49: 270-297.