See other cases
Cecal sessile polyp (LST-G)
History :
A 52-year-old woman presented for colonoscopic evaluation, performed as part of an opportunistic screening program.
Clinical & biological :
Within normal limits.
Imaging :
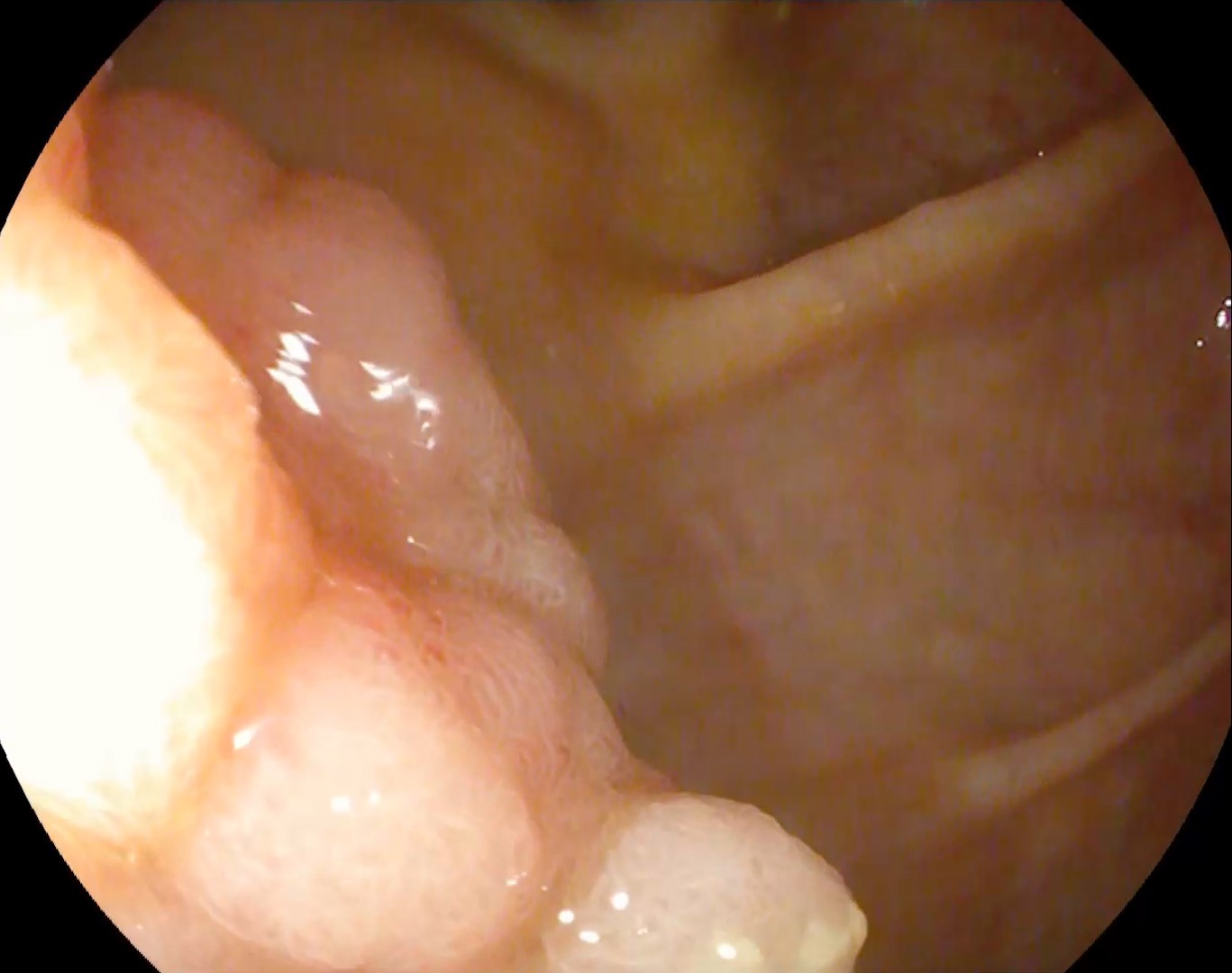
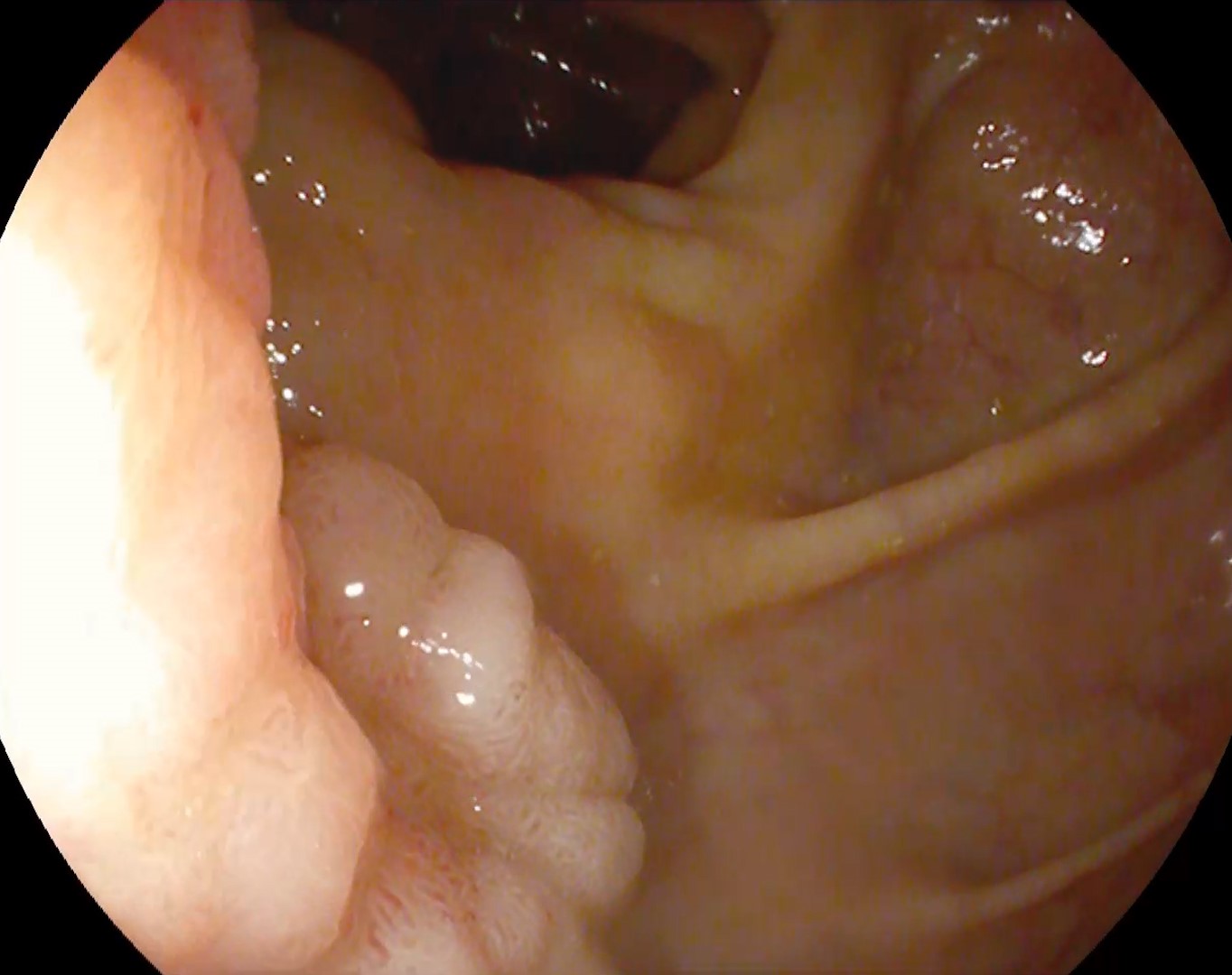
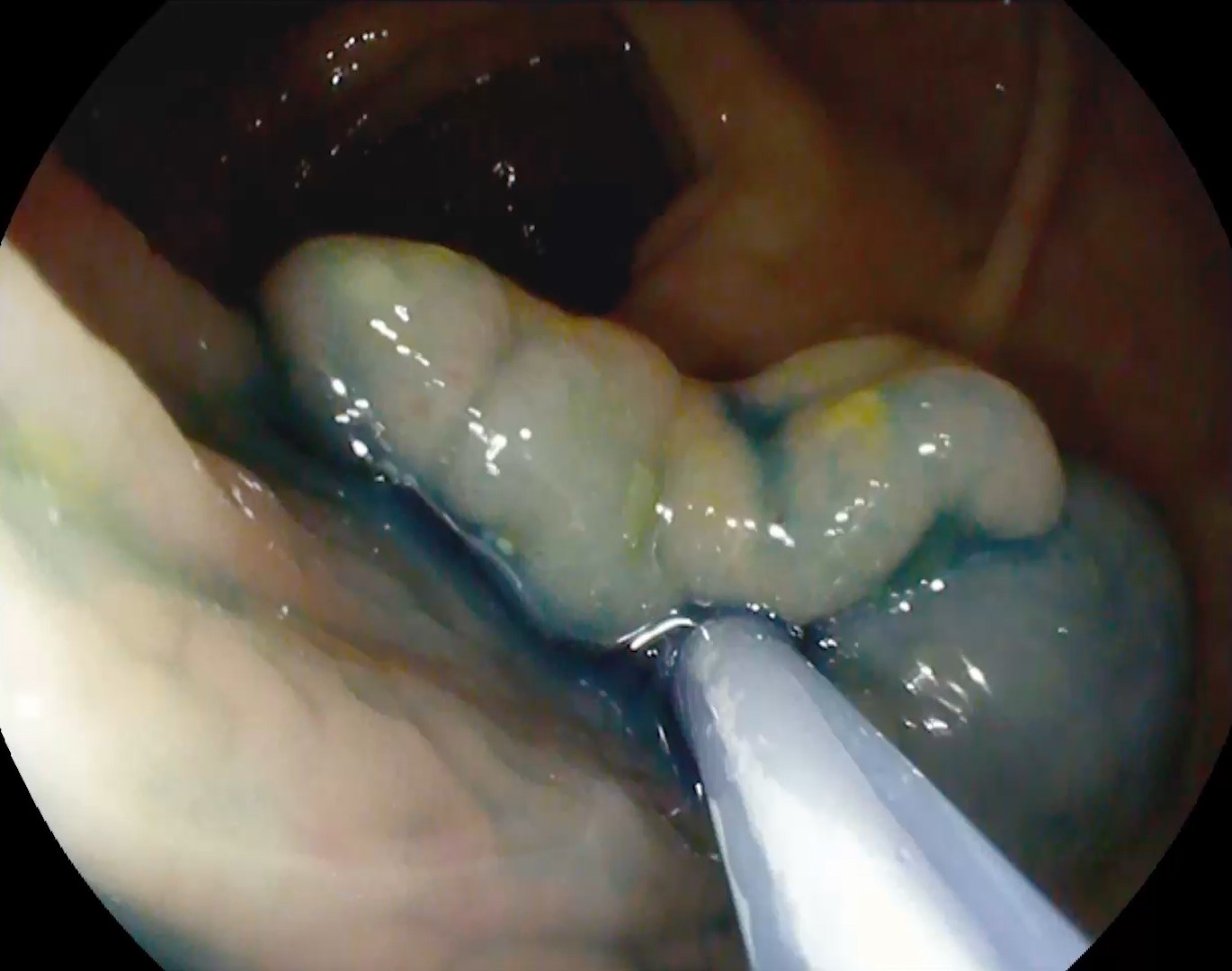
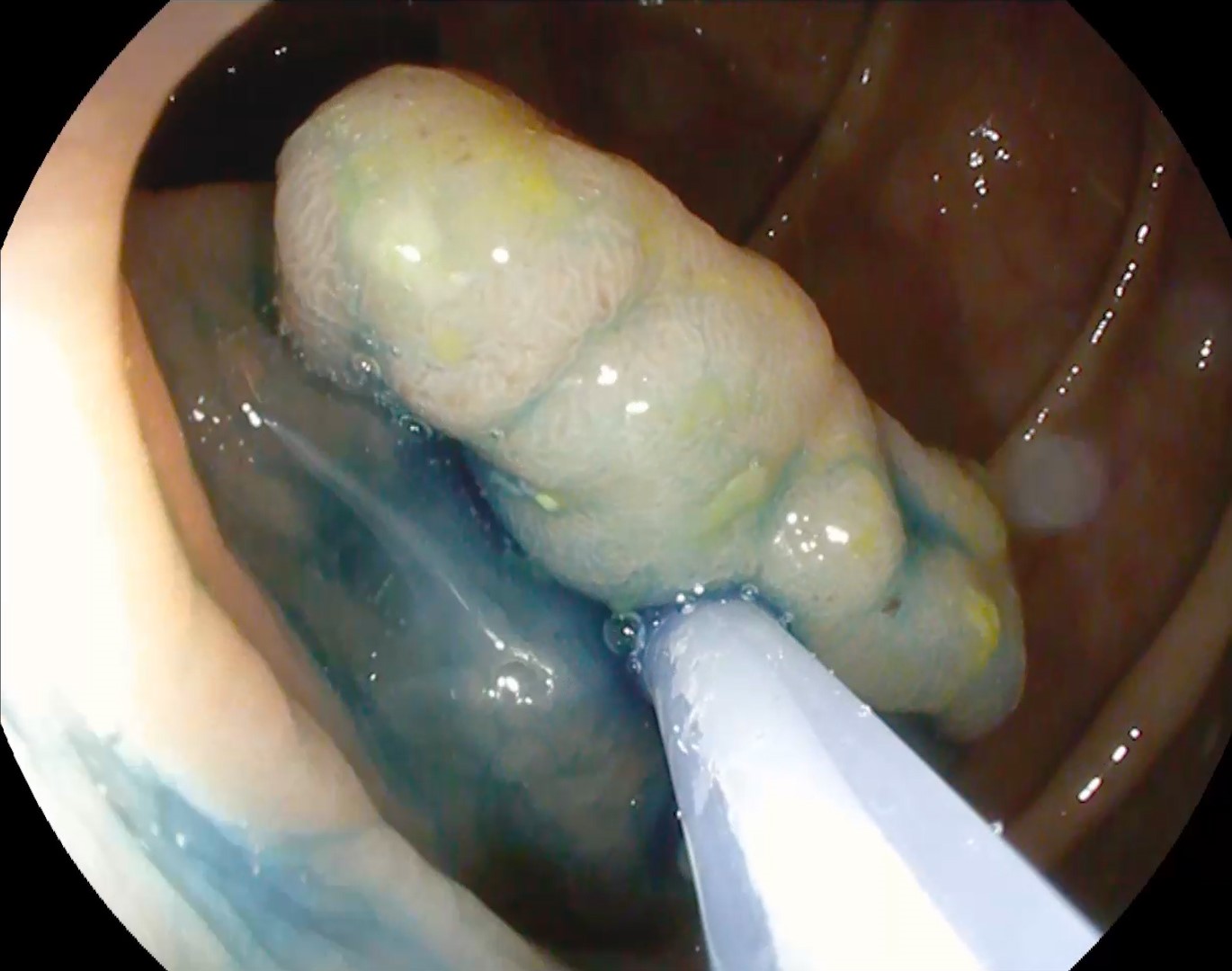
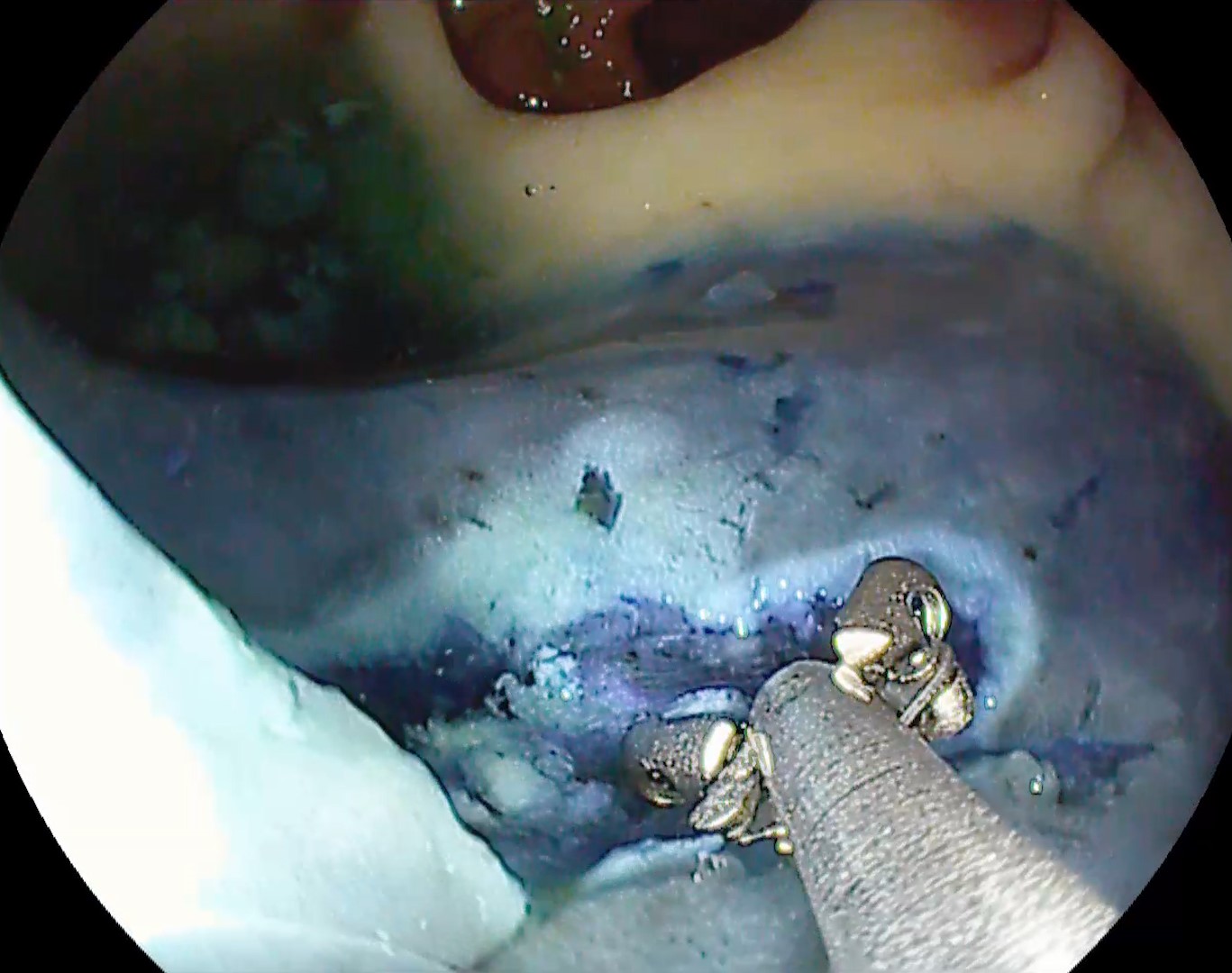
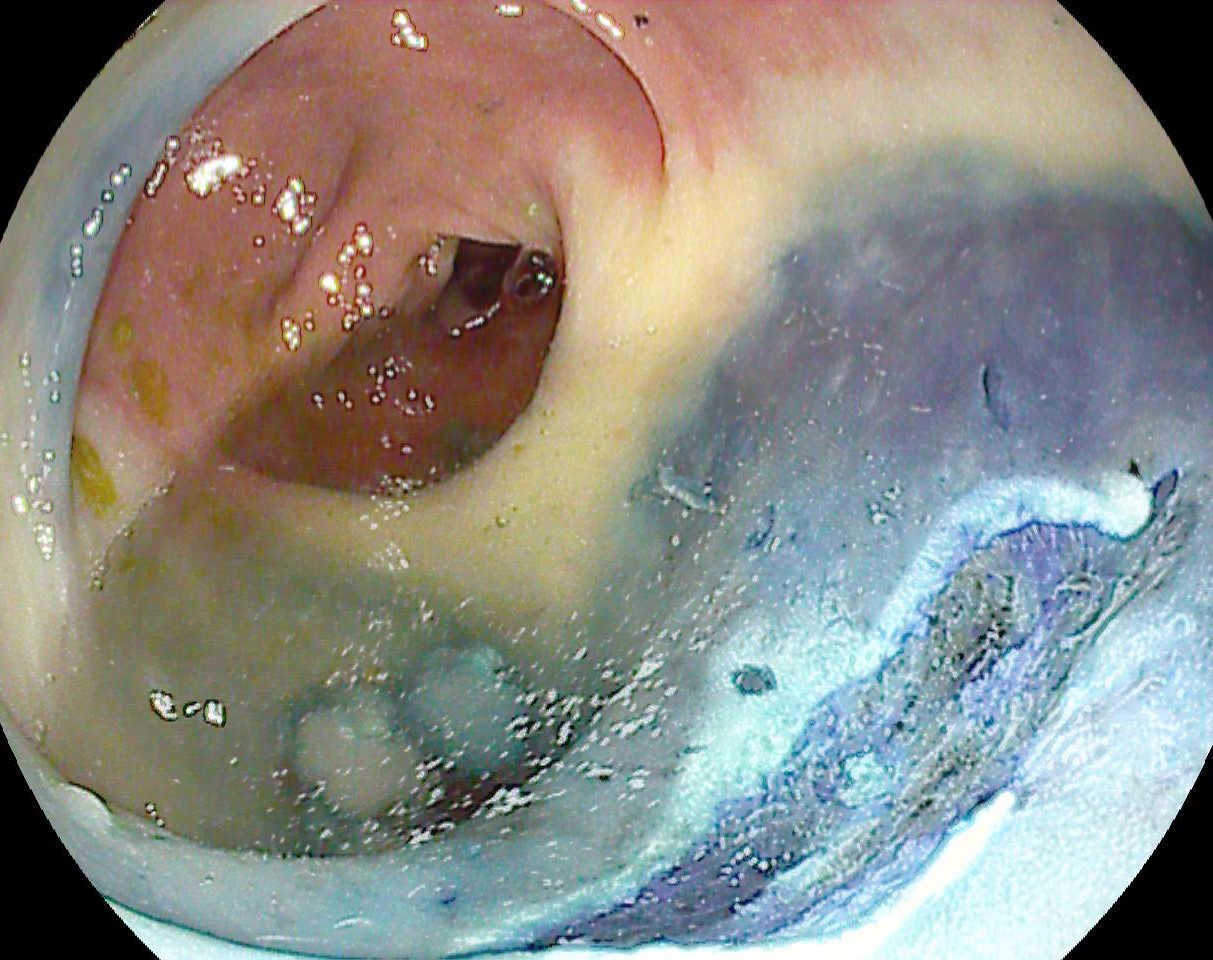
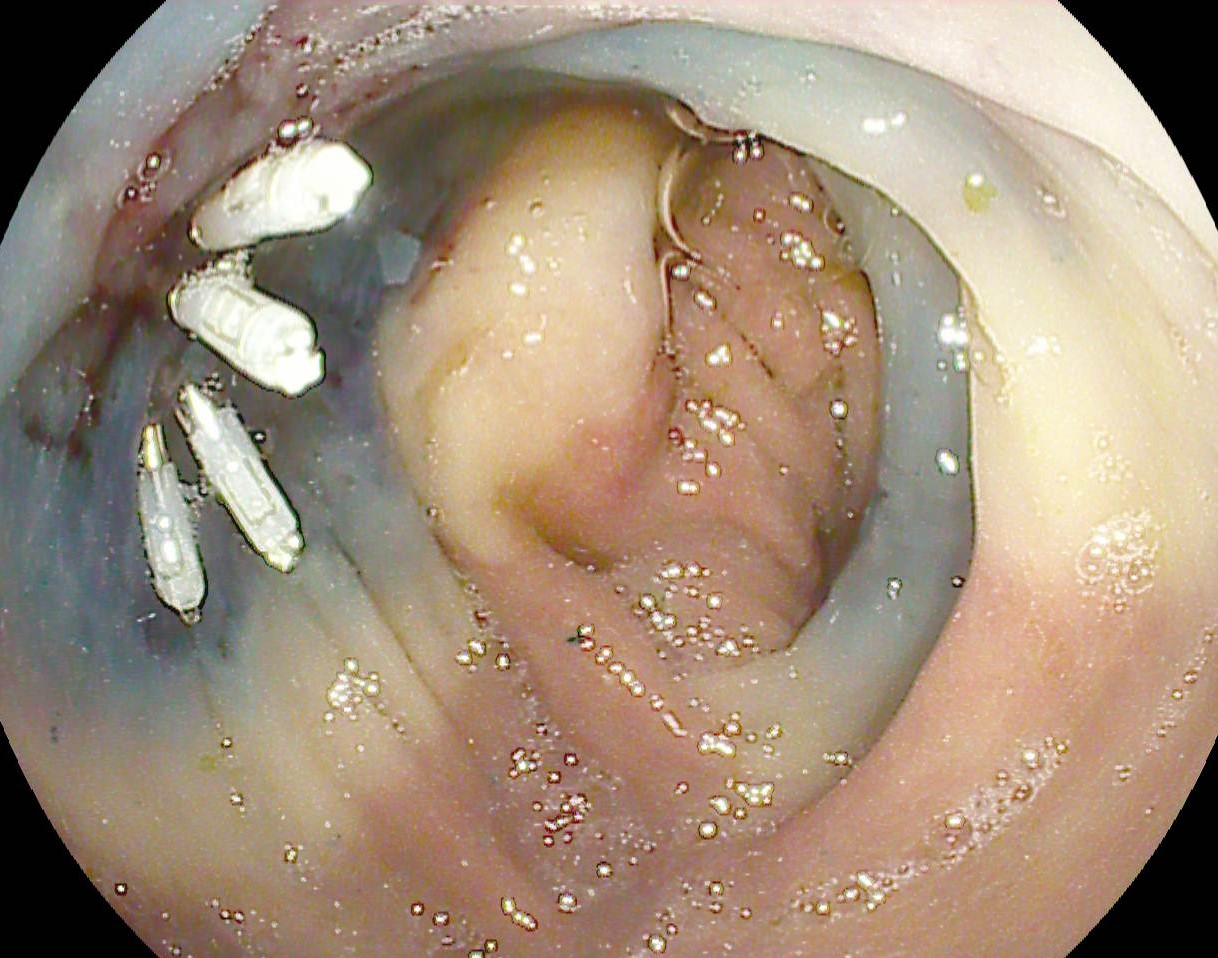
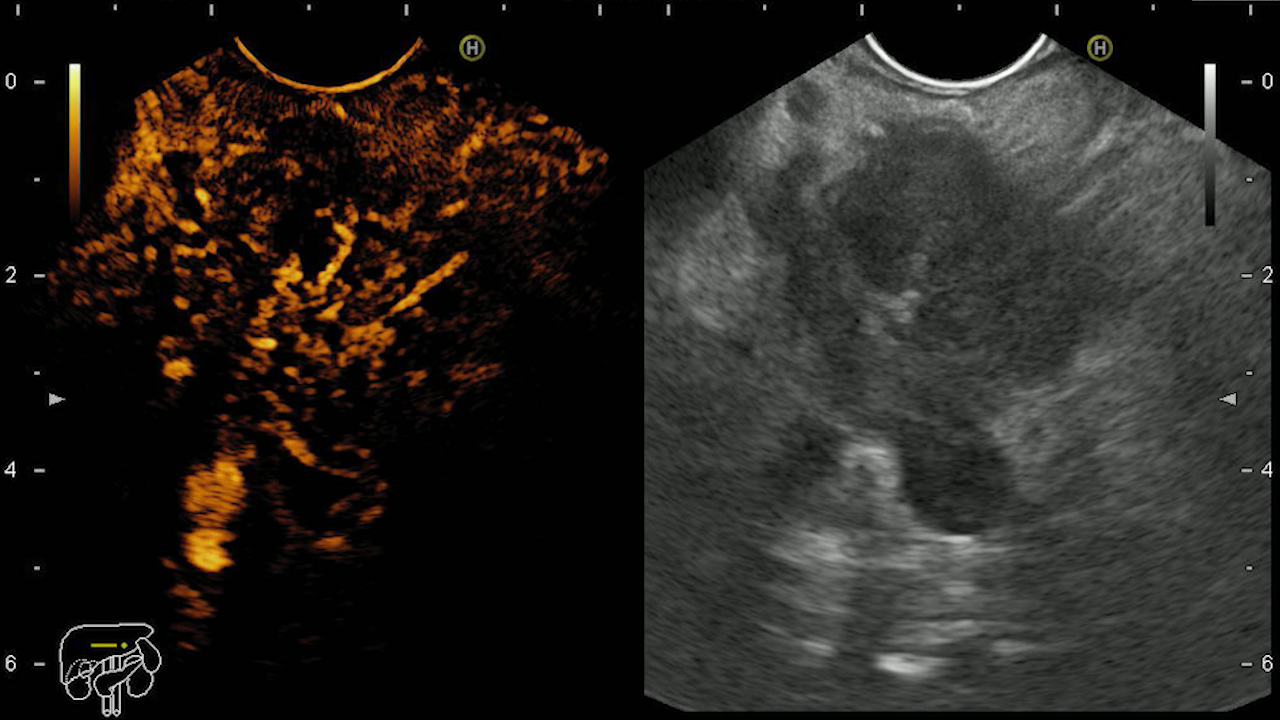
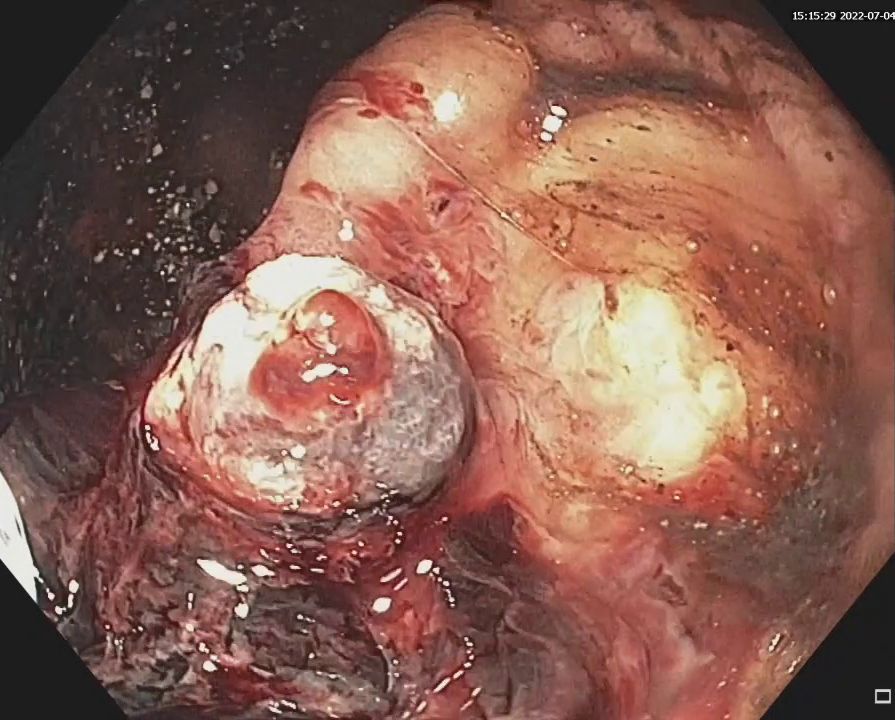
Colonoscopy identified a sessile granular LST-G (lateral spreading tumor – granular type) lesion of approximately 30 mm in diameter, Paris 0-IIa, J-NET 2A (NICE 2) located immediately above the ileo-cecal valve. Taking into account the low risk of submucosal invasion of the lesion (< 0.5%), piece-meal endoscopic mucosal resection (pEMR) was performed, associated with cold avulsion and coagulation with the tip of the snare (cold -forceps avulsion and adjuvant snare-tip soft coagulation – STSC) (Figure 1-3, Film 1). The fragments were recovered with a mesh loop for histopathological examination. The defect was closed with hemostatic clips with a rechargeable device.
Diagnostic :
The diagnosis was established based on the histopathological examination, which confirmed the presence of a tubulovillous adenoma with high-grade dysplasia, without submucosal invasion and with no adenocarcinoma foci.
Discussion :
pEMR is the primary technique of choice for resection of LST-G lesions because visual feedback allows real-time assessment of immediate bleeding and the edges of the resulting defect or vessels can be coagulated1,2. Variants of the method include the use of elastic ligatures (lEMR ) or performing the procedure underwater (uEMR)3,4. The use of snare-tip coagulation reduces the risk of bleeding and, respectively, the risk of recurrence5. However, endoscopic submucosal dissection (ESD) techniques are superior for complete and en-bloc resection rates, with lower recurrence rates6.
Conclusion :
Piecemeal endoscopic mucosal resection (pEMR) is considered a useful technique for resection of LST lesions, especially if ESD expertise is not available.
References :
- Guarner-Argente C, Ikematsu H, Osera S, Fraile M, Ibañez B, Marra-López C, et al. Location, morphology and invasiveness of lateral spreading tumors in the colorectum differ between two large cohorts from an eastern and western country. Gastroenterol Hepatol 2022; 45: 440-449.
- Tate DJ, Bahin FF, Desomer L, Sidhu M, Gupta V, Bourke MJ.Cold-forceps avulsion with adjuvant snare-tip soft coagulation (CAST) is an effective and safe strategy for the management of non-lifting large laterally spreading colonic lesions.Endoscopy 2018;50:52-62.
- Kichler AJ, Diehl DL.Wide-field endoscopic mucosal resection of laterally spreading rectal tumors using a multiband ligation endoscopic mucosal resection technique.VideoGIE 2021;7:53-57.
- Matsueda K, Takeuchi Y, Ishihara R.Underwater endoscopic mucosal resection for a laterally spreading tumor involving the ileocecal valve and terminal ileum.Dig Endosc 2021;33:206.
- Chandan S, Facciorusso A, Ramai D, Deliwala S, Mohan BP, Kassab LL, Draganov PV, Othman MO, Kochhar GS.Snare tip soft coagulation (STSC) after endoscopic mucosal resection (EMR) of large (> 20 mm) non pedunculated colorectal polyps: a systematic review and meta-analysis.Endosc Int Open 2022;10:E74-E81.
- Zhao HJ, Yin J, Ji CY, Wang X, Wang N.Endoscopic mucosal resection versus endoscopic submucosal dissection for colorectal laterally spreading tumors: a meta-analysis. Rev Esp Enferm Dig 2020;112:941-947.