See other cases
Benign post-operatory esophago-gastric anastomotic stenosis
History :
A 59-year-old male with a history of surgery for esophageal neoplasm in 2019 (Ivor Lewis technique: intrathoracic esophago-gastric anastomosis), presents complaining of mixed dysphagia. In the previous two years the patient underwent multiple endoscopic dilations with multi-diameter balloon and Savary bougies. Repeated biopsies of the anastomosis did not exhibit any sign of malignancy.
Clinical & biological :
His clinical examination and blood work did not reveal any abnormalities.
Imaging :
A barium swallow examination was requested which revealed a dilated remnant of esophagus along with a tight esophago-gastric anastomosis and normal gastric stump (Fig. 1) and duodenum.
The full-body CT scan with contrast did not show any abnormal adenopathy or distant metastasis.
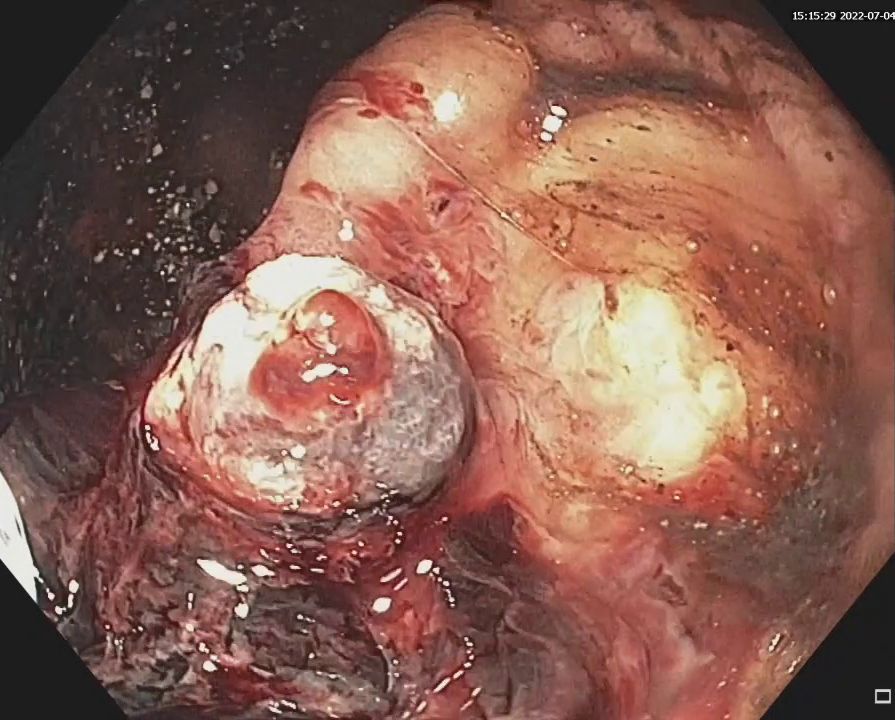
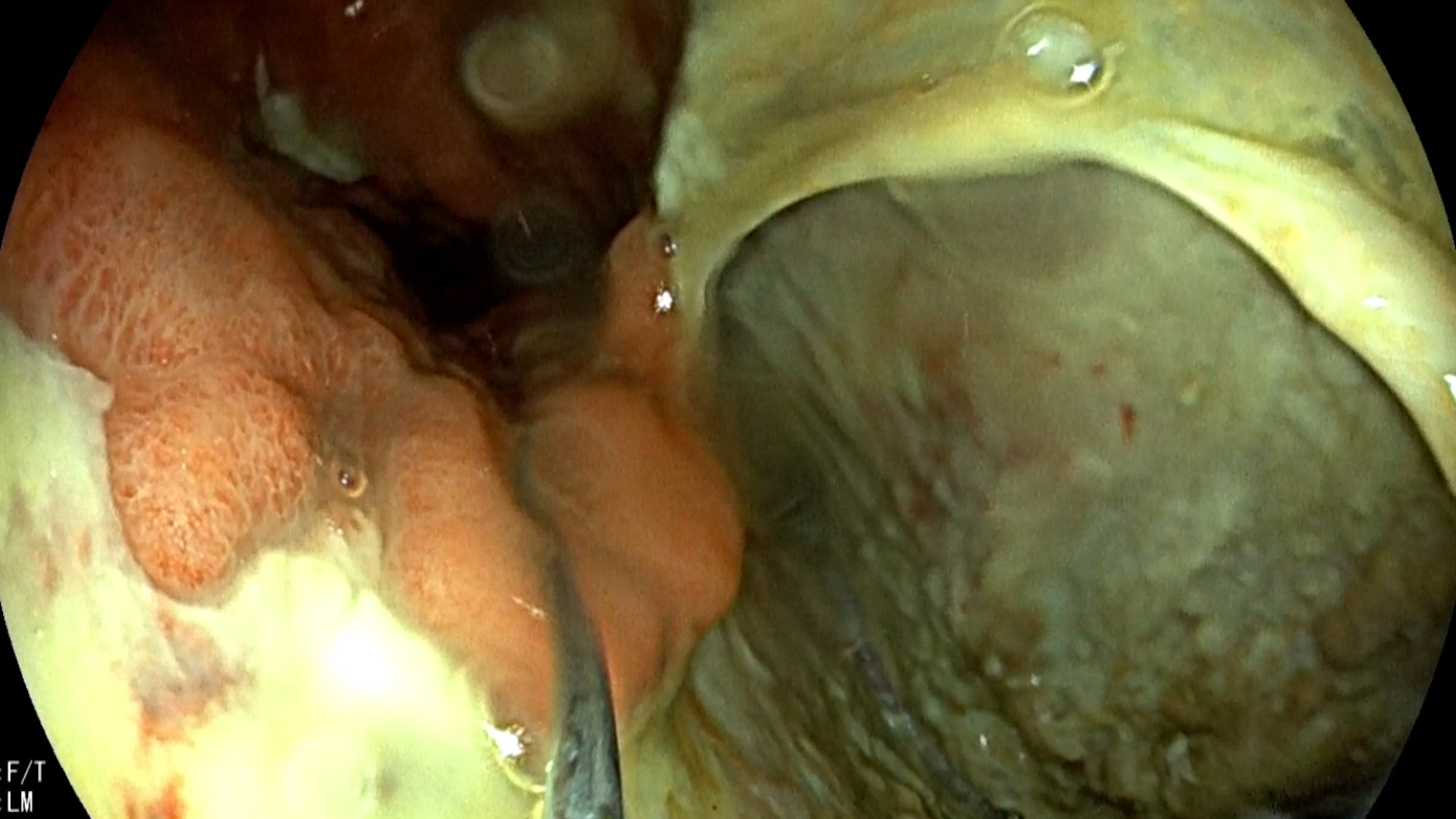
Upper GI endoscopy was performed and unveiled an unpassable esophago-gastric anastomotic stricture at approximately 24 cm from the incisors (Fig. 2).
Diagnostic :
Benign post-operatory esophago-gastric anastomotic stenosis.
Discussion :
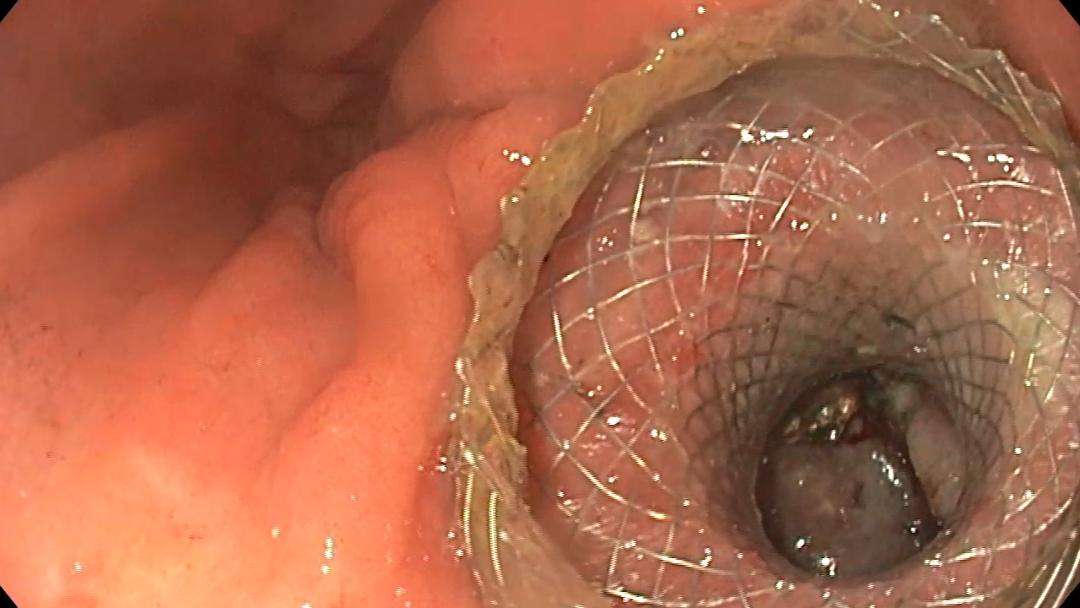
Incisional therapy with needle knife (Fig 3) was performed followed by placement of a 22/10 mm fully covered esophageal stent. Barium swallow with non-ionic contrast at 24 h after the procedure revealed a calibrated anastomotic stenosis with appropriate placement of the esophageal stent. No fistula tract was observed. (Fig 4). The patient was discharged the next day. At 4 weeks after the placement of the esophageal stent the patient was admitted for its extraction. Upper GI endoscopy revealed a calibrated esophago-gastric anastomosis.
The benign post-operatory esophago-gastric anastomosis has multiple options for endoscopic treatment:
- Multi-diameter balloon and Savary bougie dilation represent the mainstray procedures for benign post-operatory anastomotic stenosis.
- Corticosteroid injection in 4 quadrants after endoscopic dilatation can be used but with limited efficacy.
- Incisional therapy with needle knife in different quadrants or placement of totally covered esophageal stents for stenosis calibration show promising results.
Conclusion :
This case illustrates the endoscopic, radiological appearance and the endoscopic management of a tight benign post operatory esophago-gastric anastomotic stenosis, refractory to endoscopic multi-diameter balloon and Savary bougie dilation.
References :
- Peter D. Siersema. Management of refractory benign esophageal strictures. Gastroenterology Hepatology 2018 Mar; 14 (3):189-191
- Simon M. Everett. Endoscopic management of refractory benign oesophageal strictures. The AdvGastrointestEndosc 2019 Jan-Dec12: 2631774519862134





Plastic is fantastic: rescue drainage with plastic stents after LAMS drainage of a pancreatic pseudocyst
Endoscopic ultrasound, Endoscopy