See other cases
Aorto-enteric fistula
History :
A 84-year-old patient with a history of high blood pressure and smoking presented to the emergency room with lower abdominal pain and marked physical asthenia. At the Emergency Department, the patient presented hematochezia.
Clinical & biological :
Clinical: hemodynamically stable, lower abdominal pain with no signs of peritoneal irritation.
Biological: WBC 32700 /microL, hemoglobin=8.1 g/dL, PLT = 321 000 /microL, INR=1.23, creatinine =1.4 mg/dl, Na=136 mmol, K=5.3 mmol, CRP = 292 mg/L, procalcitonin = 2.32 ng/mL.
Imaging :
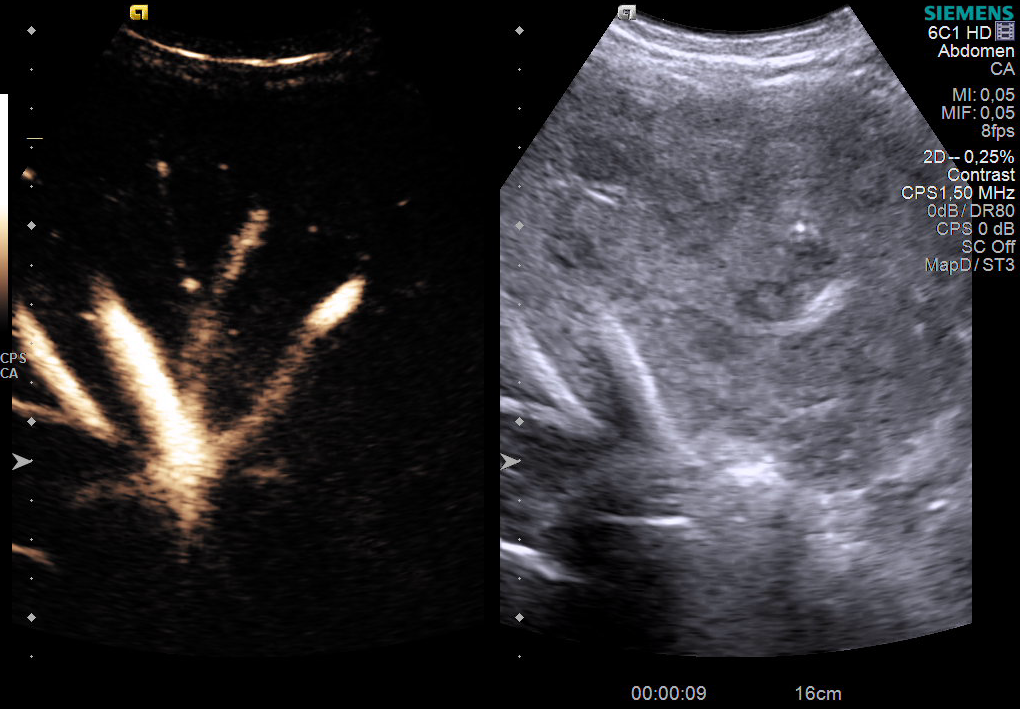
Given the symptoms, it was decided to urgently perform a CT scan with contrast:
– No contrast extravasation in the digestive tract, instead: infrarenal aortic aneurysm (130 mm cranio-caudal), with parietal thrombus, cuffed by a collection suggestive of a retroaortic abscess
– The aneurysm + the collection formed a forceps that almost completely stenoses the inferior vena cava; superior mesenteric artery with severe atheroma and thready flow.
Diagnostic :
A vascular surgery consultation was initially performed: no surgical indication at the moment and admission to the gastroenterology department was decided. Emergency upper GI endoscopy revealed a large adherent clot in the fornix and stasis fluid (penetrating to approx. 5-6 cm of D2). A 60 cm rectosigmoidoscopy was also performed: mucosal lesions compatible with the diagnosis of ischemic colitis.
Paraclinical reevaluation after 12 h: WBC = 26 000 /microL, hemoglobin = 7.1 g/dL
Taking into consideration that the source of the upper bleeding was uncertain: re-evaluation of the CT scan images showed the absence of the demarcation line between the inferior duodenal angle and the aneurysmal wall, with the suspicion of a possible aorto-duodenal fistula (Figure 2 + 3).
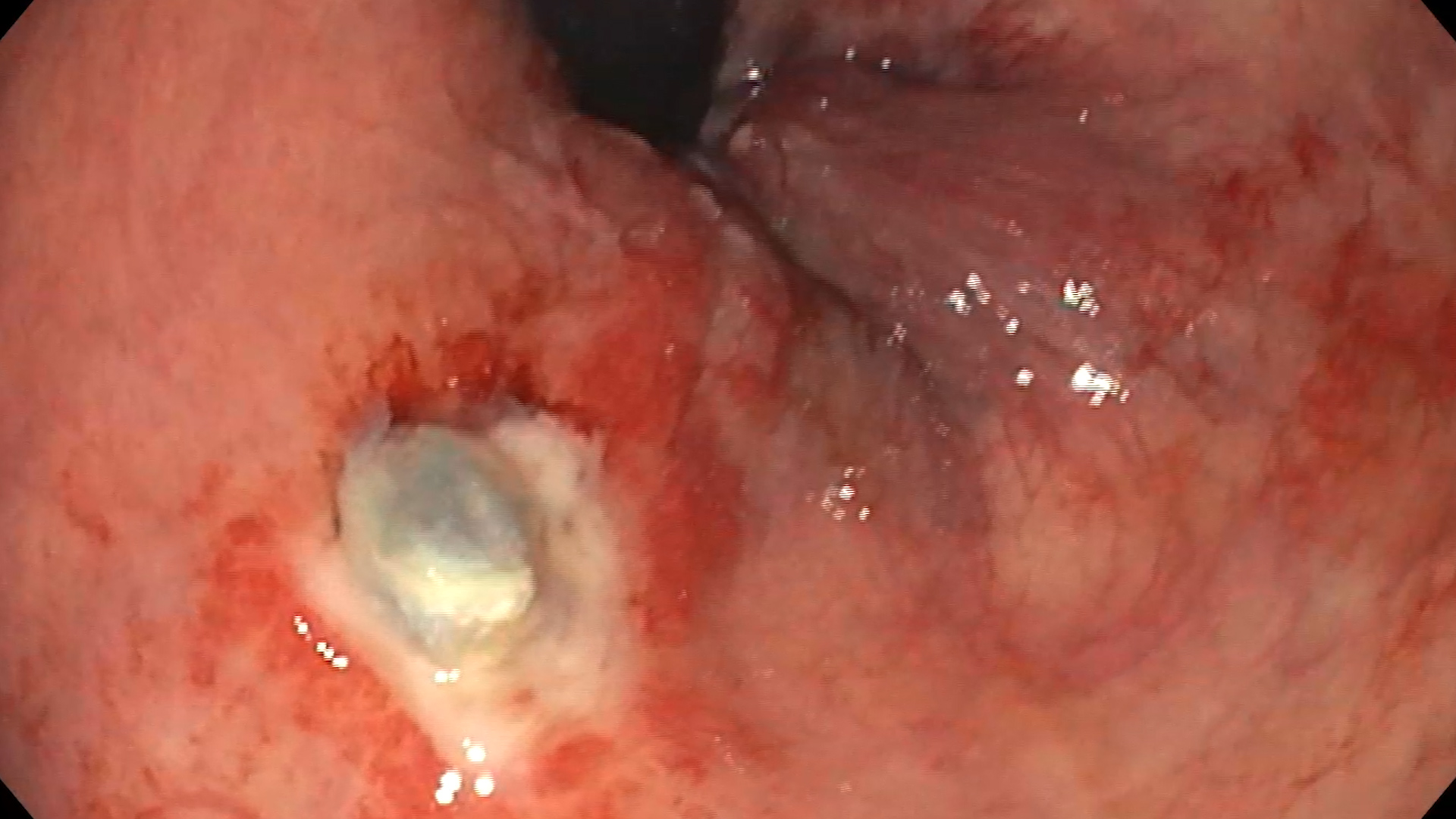
Upper GI endoscopy after 12 h: a clot at the level of the fornix, with no underlying lesion; gastric mucosa was lined with fresh blood; the bulb and D2 appeared covered with fresh blood. On withdrawal, an infrapapillary lesion suggestive for an aorto-enteric fistula was visualized with difficulty. It was re-examined with the duodenoscope that revealed the lesion: erosion with a diameter of approx. 10-12 mm with a deep punctate hole – in the clinical and imaging context, most likely aortoenteric fistula (Figure 1).
The patient was transfered to the cardio-vascular surgery section, Fundeni Clinical Institute. Emergency surgery was performed to remove the aneurysm of the infrarenal abdominal aorta and the fistula, double-layer duodenorrhaphy and aorto-aortic interposition of a silver Dacron prosthesis (Figure 4).
Discussion :
Aortoenteric fistula is a rare cause of frequently fatal gastrointestinal bleeding, difficult to diagnose. Mortality is approximately 77% with treatment and 100% without treatment. Most often the fistula occurs at the duodenal level. Aortoenteric fistulas are of 2 types:
1. Primary: most often an aneurysm with compression of the digestive tract, tumors, foreign bodies, radiotherapy
2. Secondary (most common): erosion after aortic graft
Conclusion :
The particularity of the case was represented by the rare cause and the difficult diagnosis of the upper digestive hemorrhage through the aortoenteric fistula. The approach and treatment required a multidisciplinary team and good cooperation / coordination between the different departments for a fast and effective treatment, often this complication of the aneurysm being fatal.
The patient was discharged after 17 days with a good general condition.
References :
1.Yang Y, Hu D, Peng D. Primary aortoesophageal fistula: a fatal outcome. Am J Emerg Med 2018; 36: 343.e1–343.e3.
2.Saers SJ, Scheltinga MR. Primary aortoenteric fistula. Br J Surg 2005; 92: 143–152.