See other cases
Giant rectal polyp
History :
A 58-year-old patient with tenesmus, fragmented stools with mucus and blood, with an insidious onset of about 6 months.
Clinical & biological :
Lower abdominal pain, rectal bleeding.
Imaging :
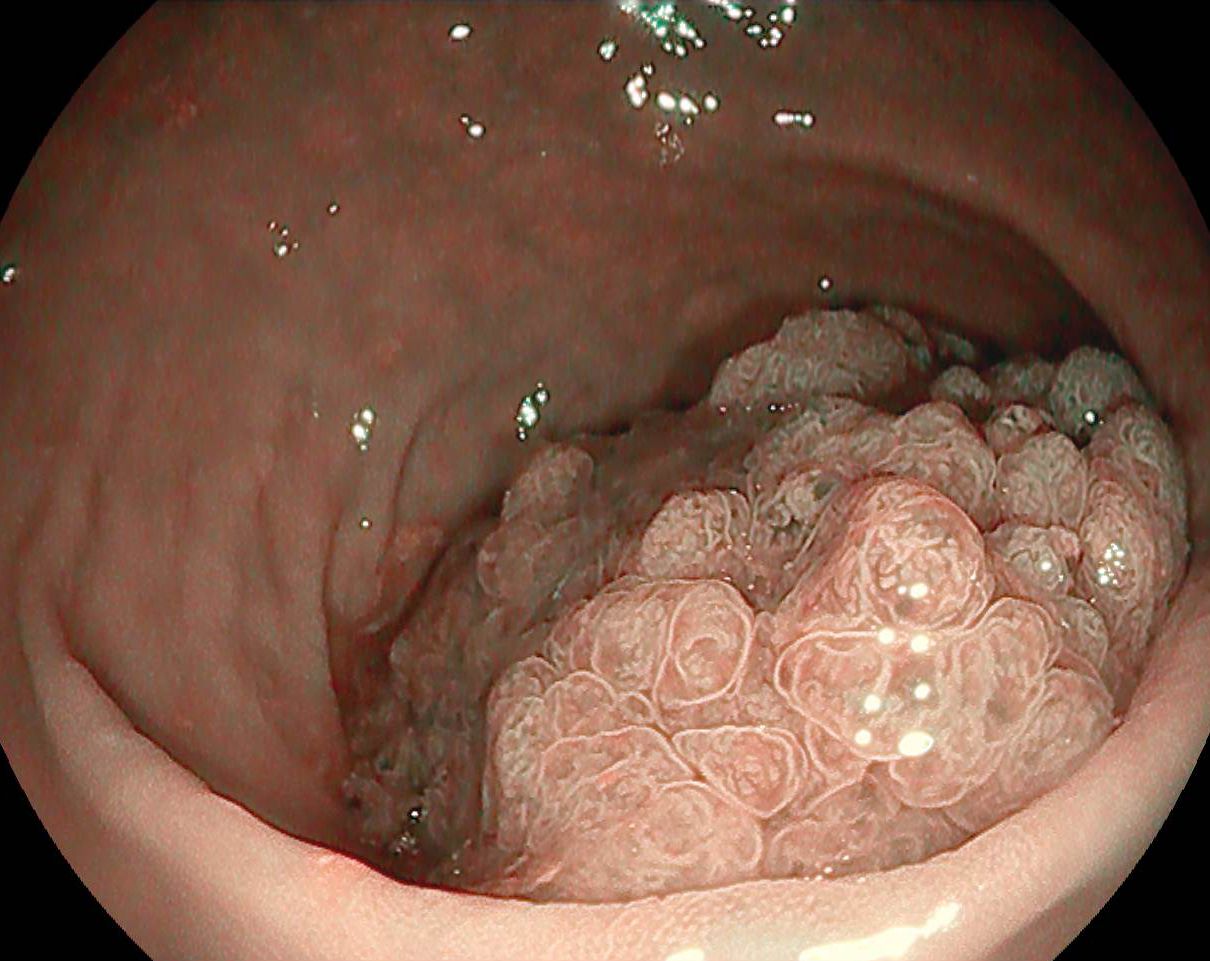
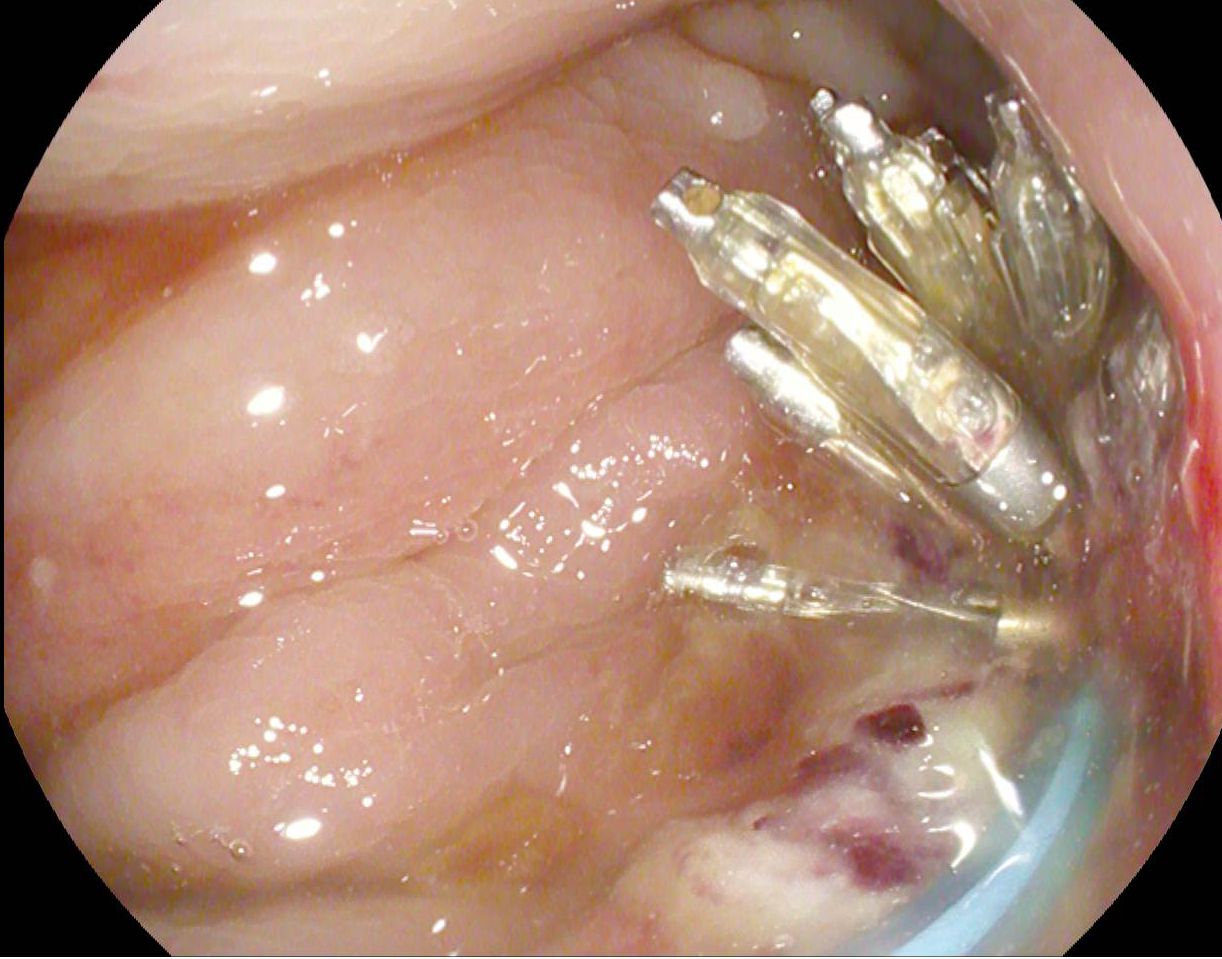
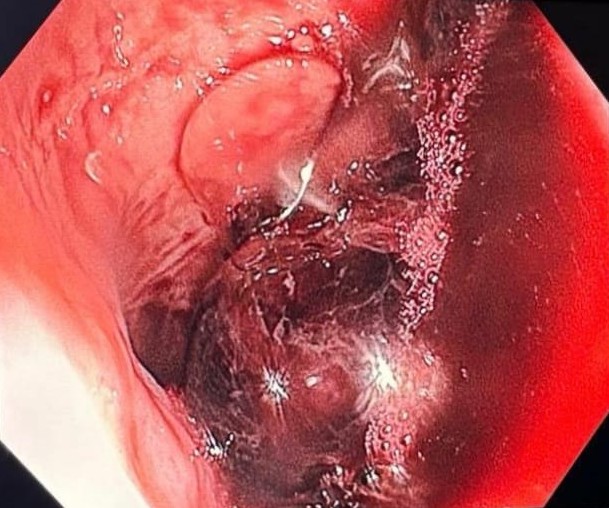
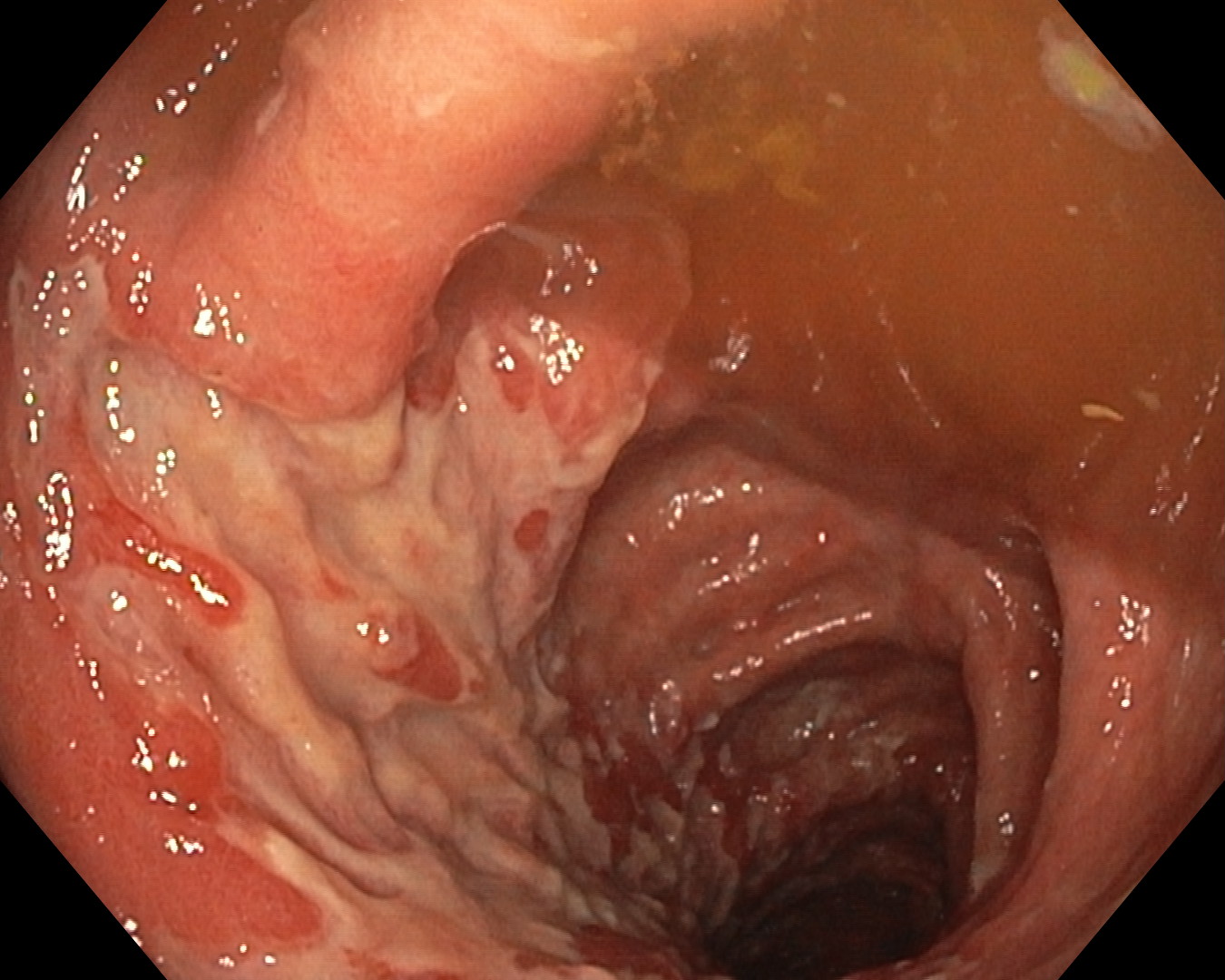
Colonoscopy revealed a semi-polypoid, vegetative mass in the lower rectum, about 5-6 cm in diameter, occupying the entire lumen, with J-NET 2B pit pattern (highlighted in white light and i-SCAN OE mode) (Figure 1-2, Movie 1). The patient refused laparoscopic / transanal surgery, being guided for endoscopic polypectomy. The polypectomy was performed in a single dominant fragment, after injection at the base of the polyp of 30 mL of 1:10 000 epinephrine diluted in Gelofusine + methylene blue (Figure 3-4, Movie 1). The result was jet bleeding (Forrest 1a), which stopped after additional injection and coagulation with coag grasper, respectively the resection of a small polypoid fragment remaining at the edge of the polypectomy (Figure 5, Movie 1). The resulting defect was closed with 8 hemostatic clips, over which an Endo-loop band was placed (Figure 5-6, Movie 1). Due to its size, the polyp was extracted using a proctoscope (Figure 7).
Diagnostic :
Tubulovillous adenoma with high-grade dysplasia, with foci of intramucosal carcinoma (intramucosal adenocarcinoma G2), with submucosal invasion (Kikutchi sm1), with a margin about 2 mm deep in muscle fibers, without perineural infiltration or lymphovascular invasion.
Discussion :
T1N0M0 malignant rectal polyps are currently treated multidisciplinary in a complex team of gastroenterologists – surgeons.
Conclusion :
The case illustrates the role of endoscopy in performing a polypectomy of a malignant rectal polyp.
References :
1. Cazacu SM, Săftoiu A, Iordache S, et al. Factors predicting occurrence and therapeutic choice in malignant colorectal polyps: a study of 13 years of colonoscopic polypectomy. Rom J Morphol Embryol 2021; 62: 917-928.
2. Ciocalteu A, Gheonea DI, Saftoiu A, et al. Current strategies for malignant pedunculated colorectal polyps. World J Gastrointest Oncol 2018; 10: 465-475.