See other cases
Endo-Endo-Looping
History :
A 53-year-old patient with a history of cirrhosis obesity and asthma, presents with nausea, vomiting, intermittent epigastric pain.
Clinical & biological :
No signs and symptoms.
Imaging :
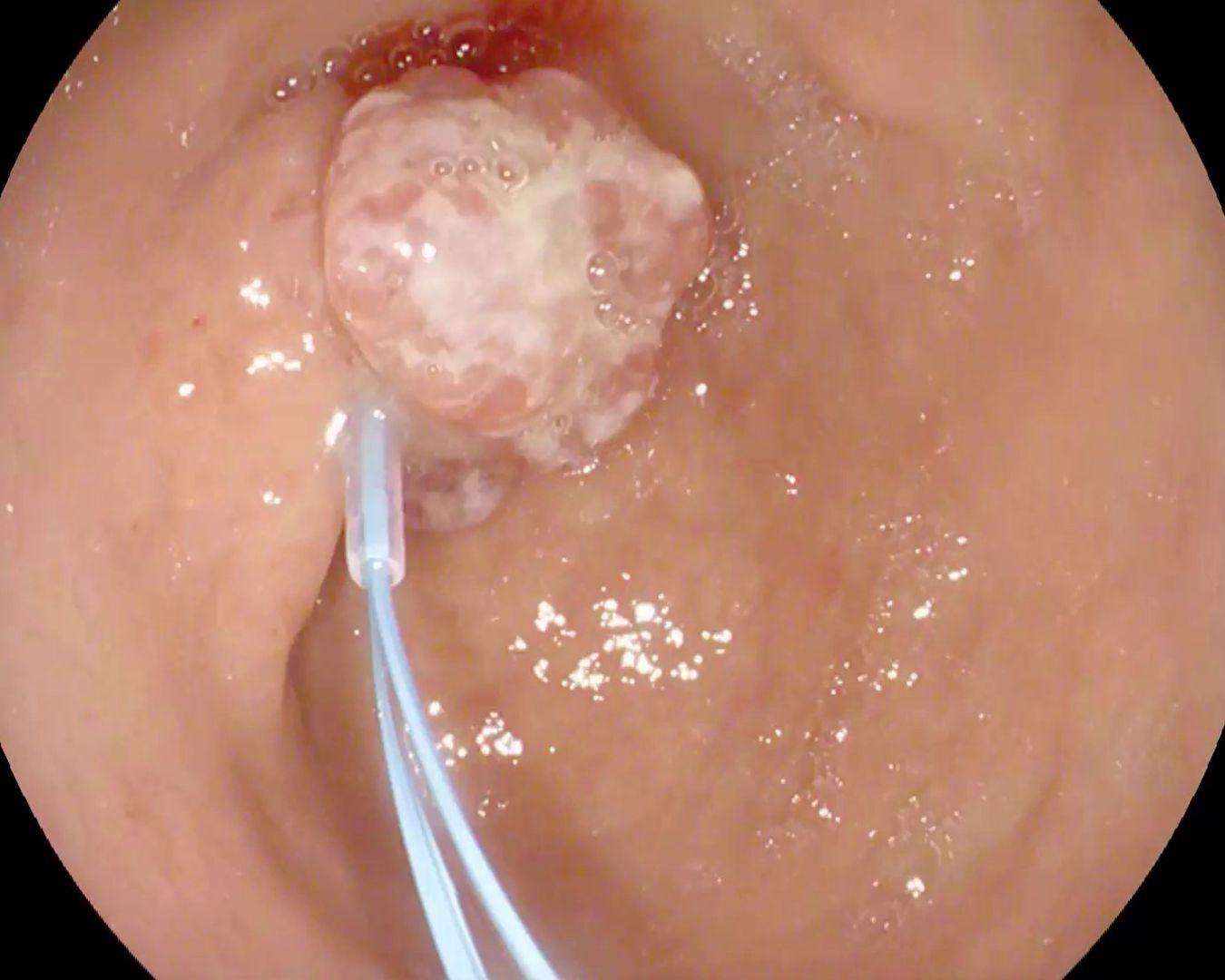
Upper GI endoscopy revealed a polypoid lesion, with a thick pedicle (> 15 mm), with hyperemia of the covering mucosa (Figure 1, Movie 1-2), classified as a Paris 1p lesion, located prepyloric. Multiple biopsies were taken, with the appearance of a hyperplastic polyp.
Diagnostic :
Prepyloric hyperplastic polyp.
Discussion :
Epithelial gastric polyps include adenomatous and hyperplastic polyps, considered precursors of early gastric cancer. Polyps are generally referred for polypectomy, especially if the patients are symptomatic and/or have foci of dysplasia. Polypectomy techniques are conventional, but generally require the use of hemostasis techniques (placement of clips / elastic bands). Due to the risk of bleeding during polypectomy, 2 elastic bands were applied, followed by removal of the polyp by self-amputation (Figure 2, Movie 1-2). The 7-day control examination revealed only a linear scar on the remaining pedicle (Figure 3).
Conclusion :
Prepyloric hyperplastic polyp, endoscopically ligated (loop-and-leave technique).
References :
1. Goddard AF, Badreldin R, Protchard DM, et al. The management of gastric polyps. Gut 2010; 59: 1270-1276.
2. Jung M. The ‘difficult’ polyp: pitfalls for endoscopic removal. Dig Dis 2012; 30 Suppl 2: 74-80.
3. Lo CC, Hsu PI, Lo GH, et al. Endoscopic banding ligation can effectively resect hyperplastic polyps of stomach. World J Gastroenterol 2003; 9(12): 2805-8.
4. Walker J, Howell DA, Gupta S, et al. Combined volume reduction with the loop-and-leave technique permits safe endoscopic management of high-risk giant gastric polyps. Gastrointest Endosc 2016; 83: 655-6.