See other cases
A rare cause of lower GI bleeding
History :
A 73 year old female patient diagnosed in another facility care with colonic Crohn disease in 2019 (at the age of 70), treated with Azathioprine for 4 years, currently with oral 5-ASA, presented at the emergency room with increase in stool frequency (5-6/day), rectal bleeding, abdominal pain and generalized edema.
The patient underwent a colonoscopy with an evaluation biopsy in December 2022, which highlighted a pseudostenosis between the ascending and transverse colon, with a secondary histopathological examination that ruled out inflammatory bowel disease.
Clinical & biological :
Clinical: fatigue, loss of appetite, generalized edema.
Biological: mild normocytic anemia (Hb: 9.5 g/dl), reactive thrombocytosis, discrete inflammatory syndrome (leukocytes: 12,000 with a predominance of neutrophils, CRP: 101mg/dl), creatinine: 1.7 mg/dl, albumin: 1.1 g/dl, urine summary: glucosuria, proteinuria (300 mg/dl).
During the hospitalisation, the pacient needed several units of blood, which is not usually found in Crohn’s disease.
Imaging :
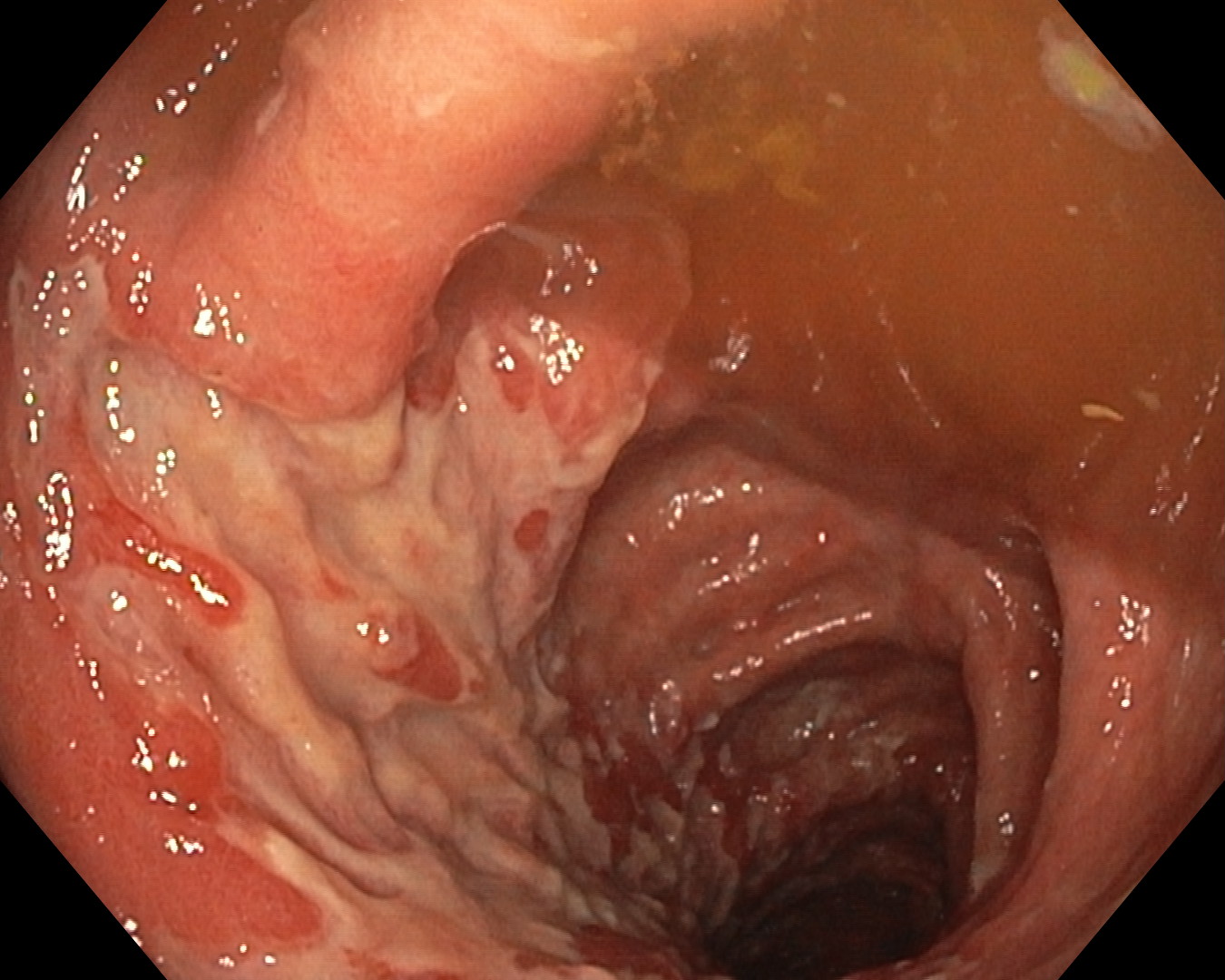
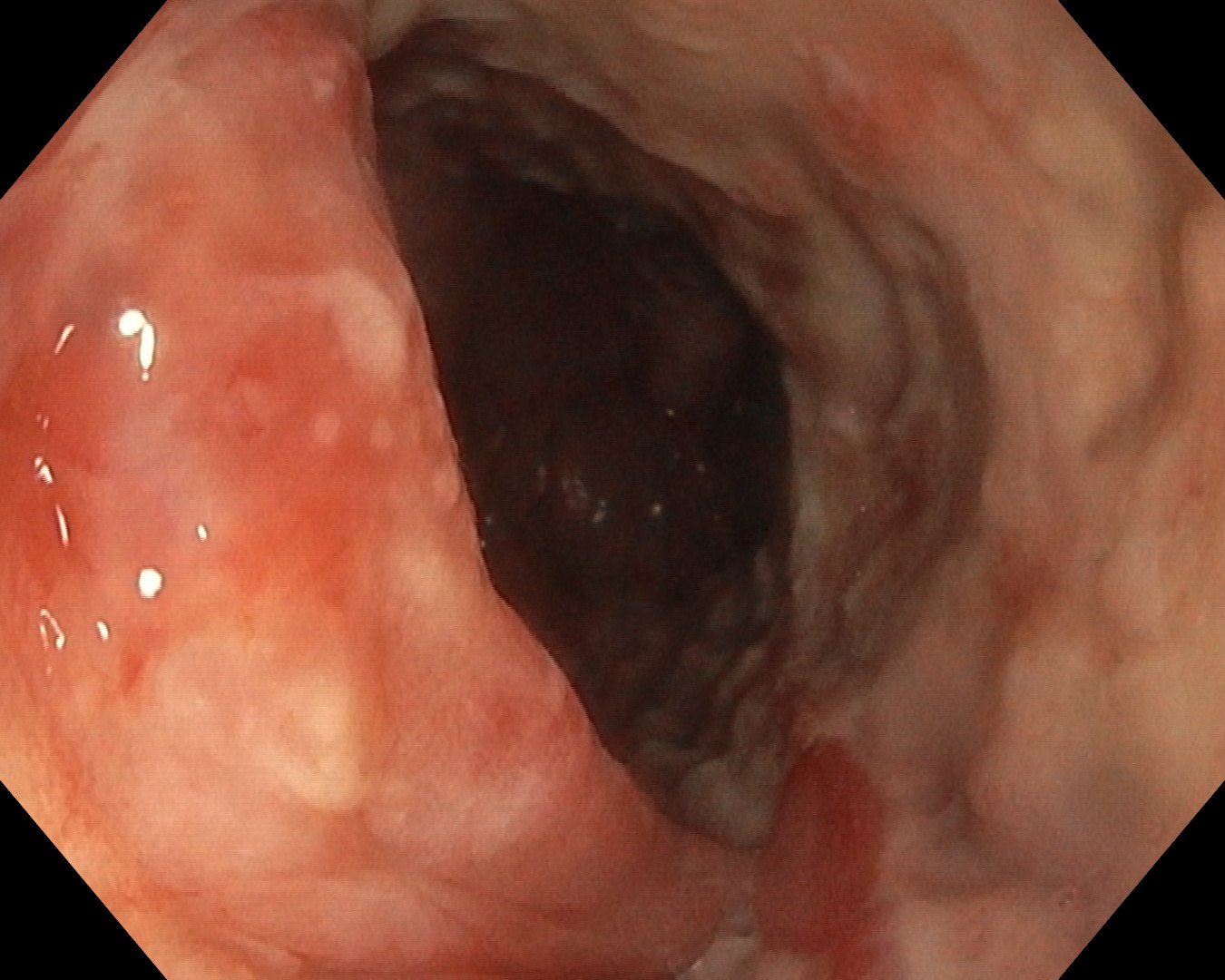
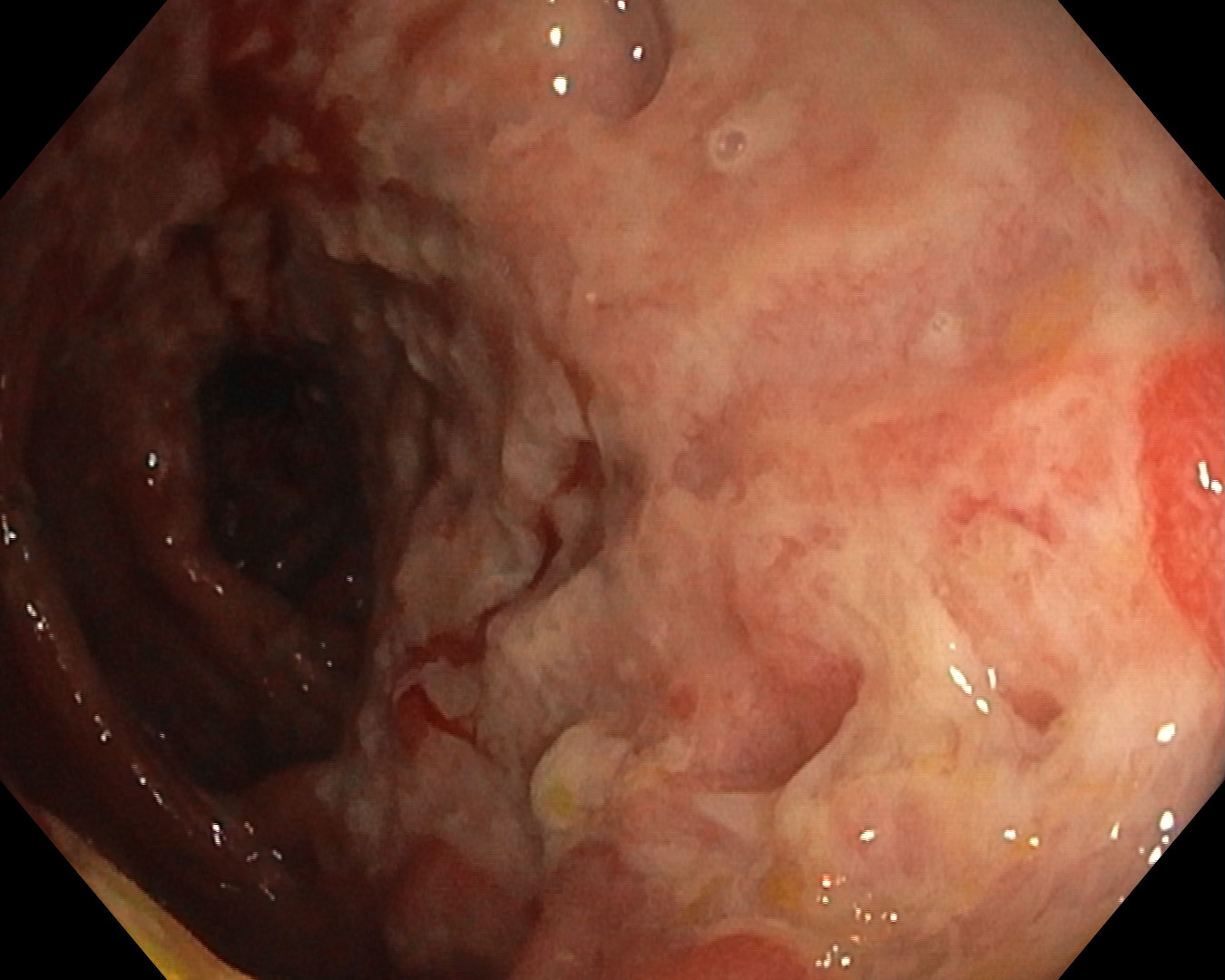
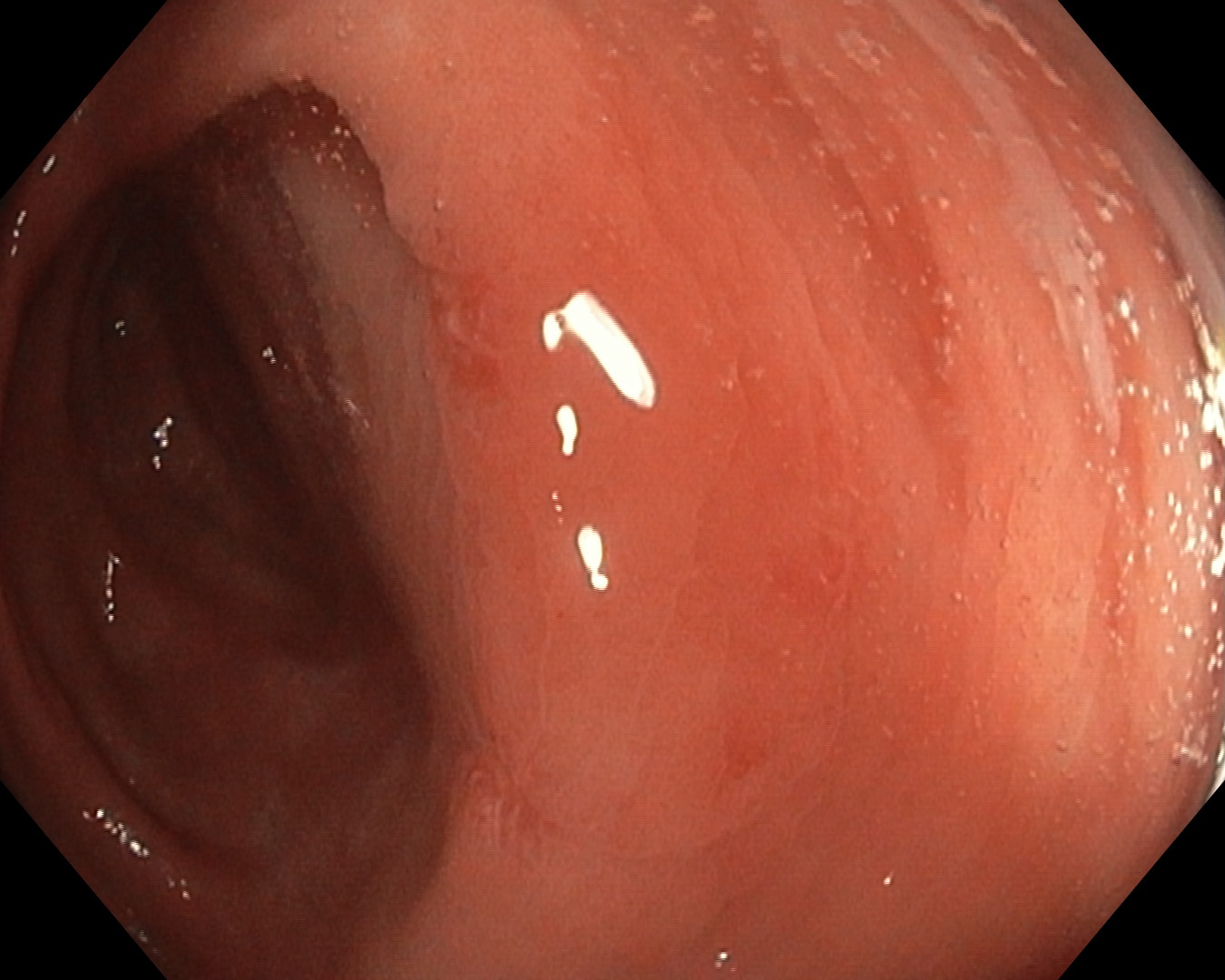
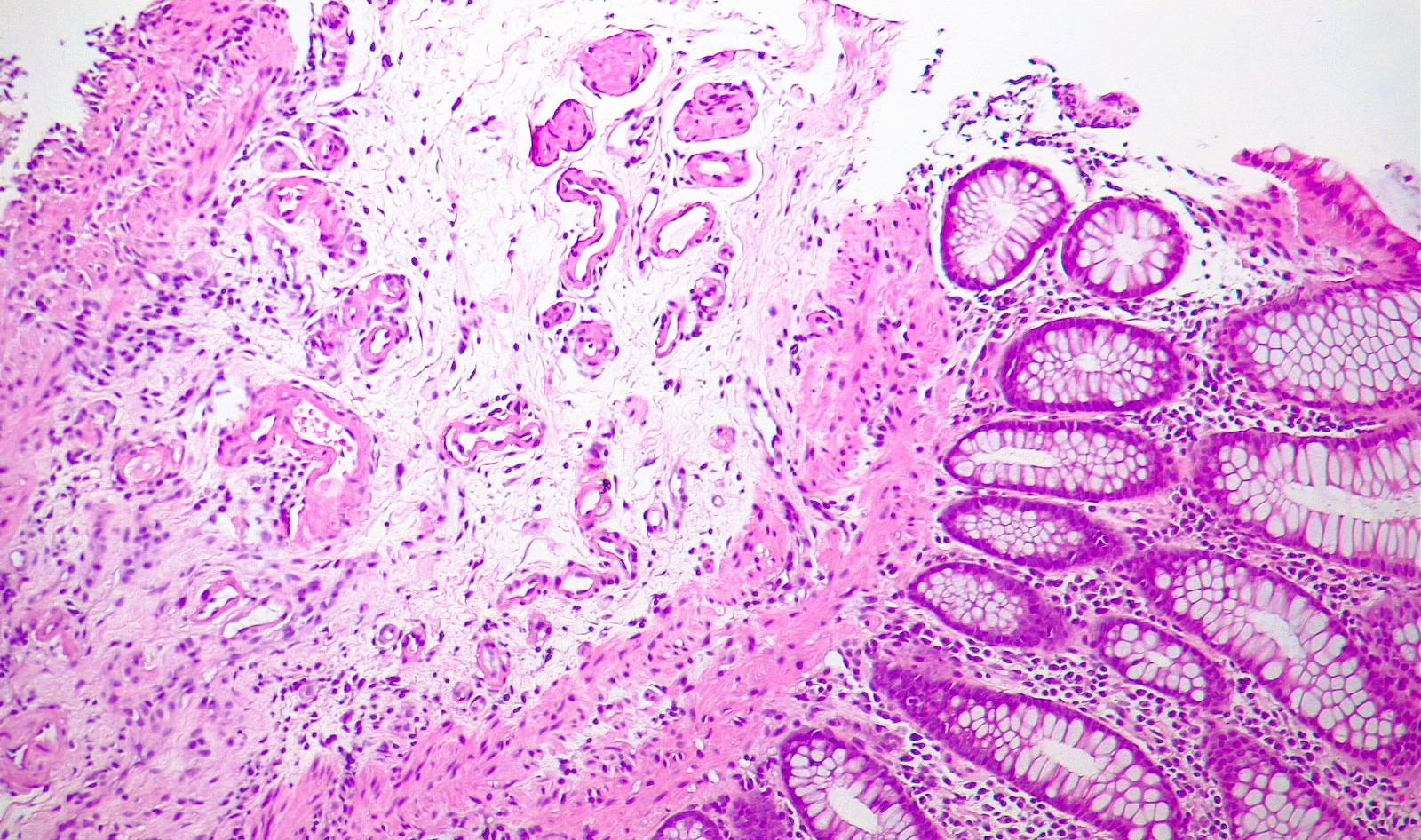
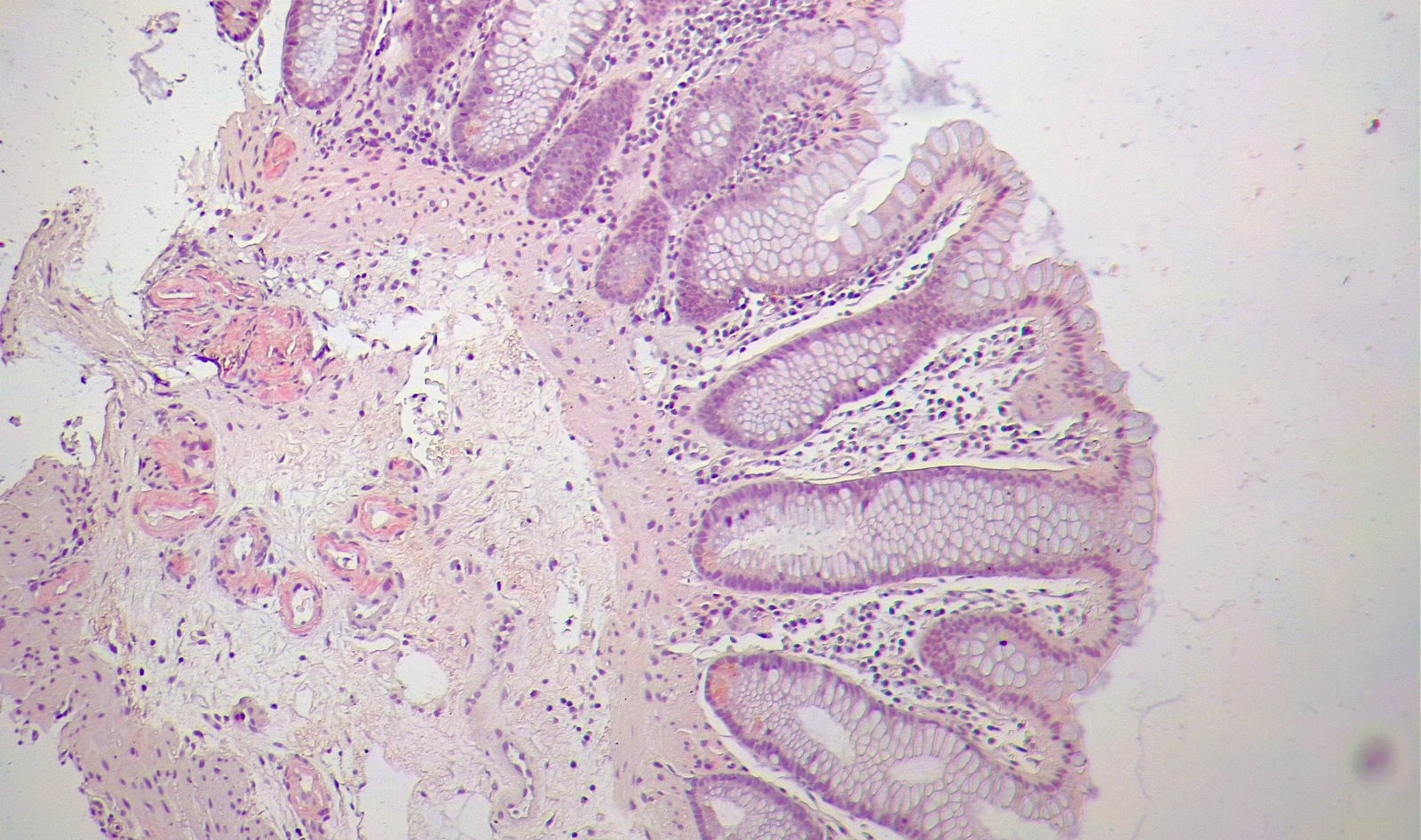
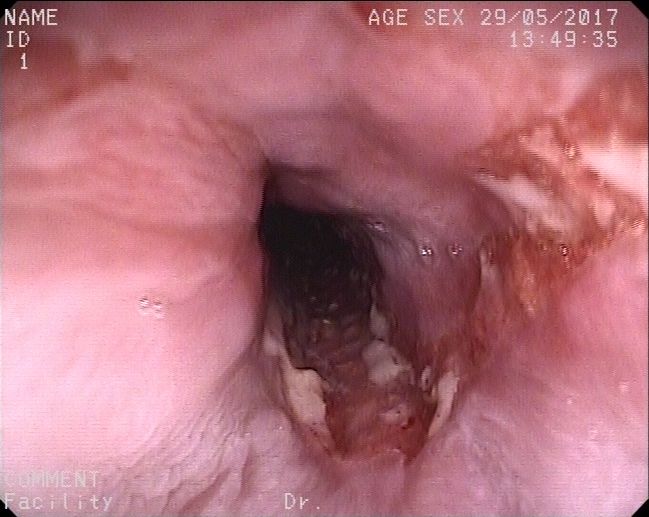
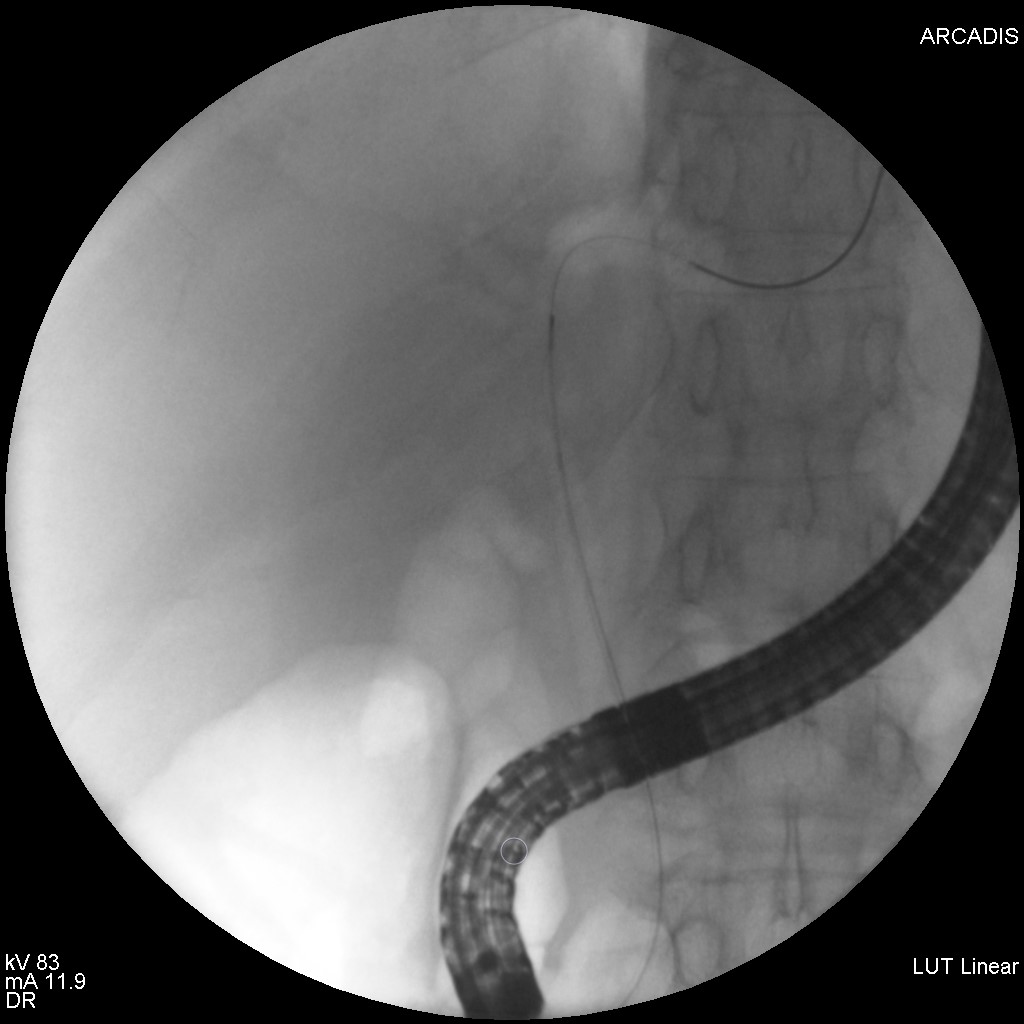
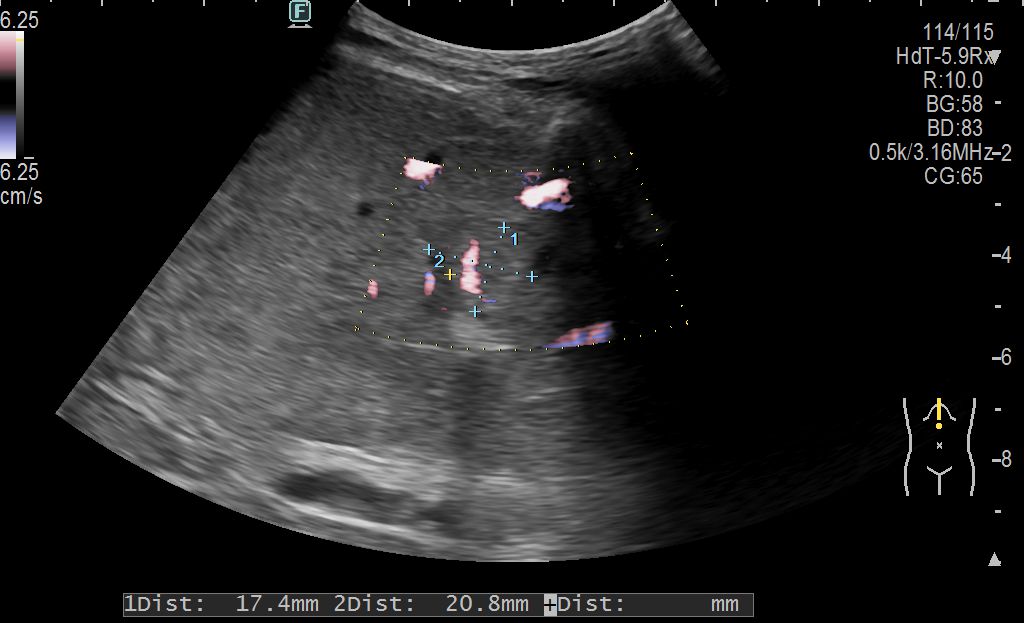
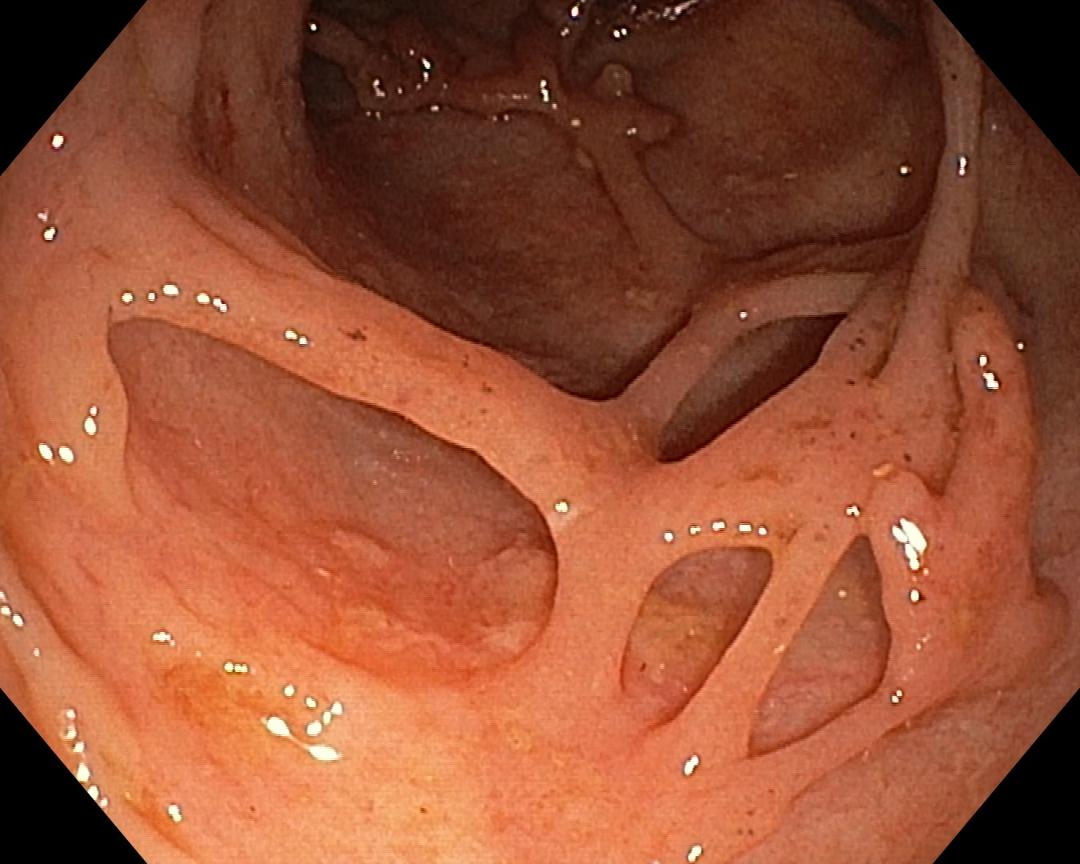
Colonoscopy: From the level of the cecum and ascending colon, there was an extensive area of denuded mucosa, alternating with areas of normal mucosa. Multiple lesions with aphthoid appearance on normal mucosa at the level of descending and sigmoid colon. Multiple biopsies were collected (Fig 1-4).
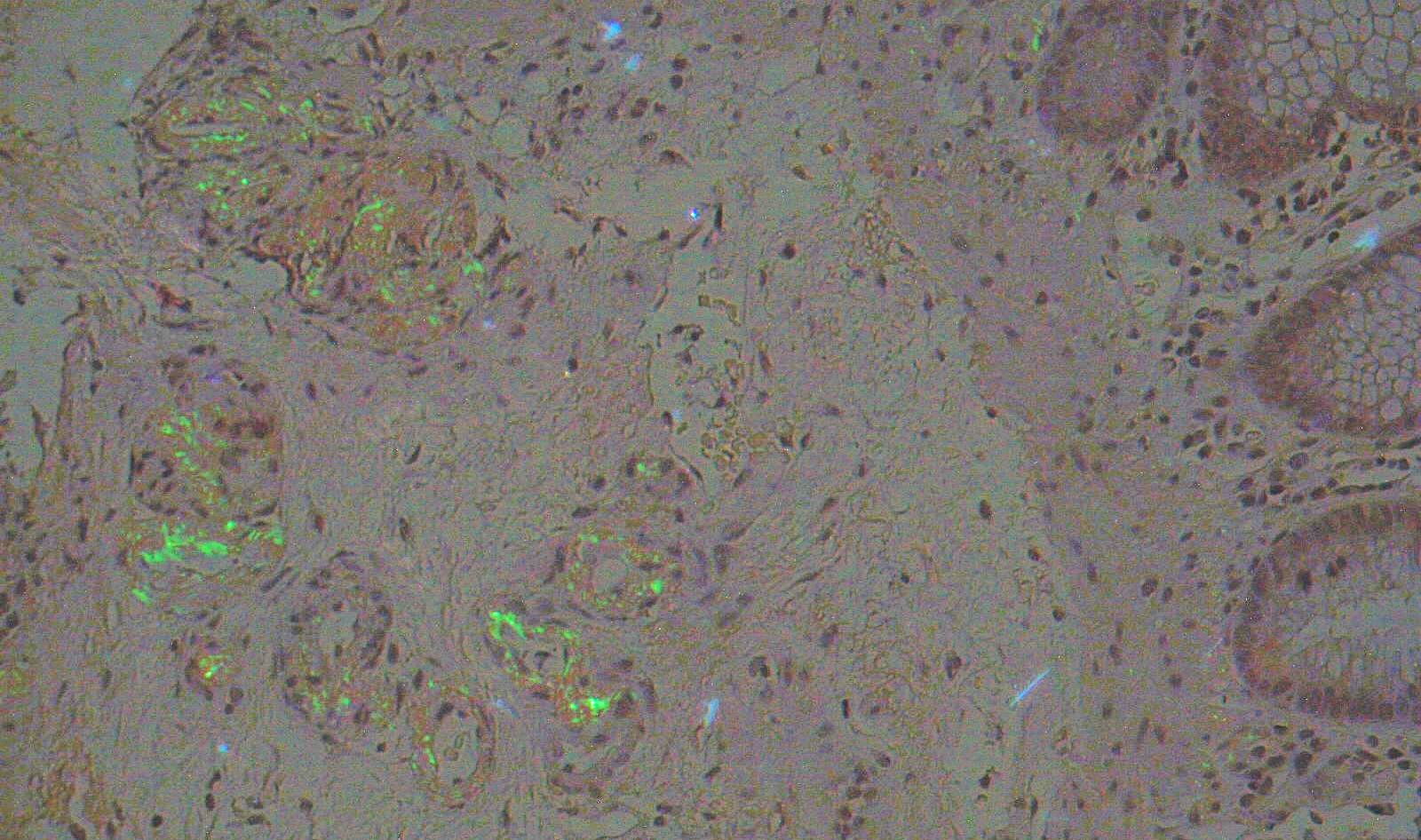
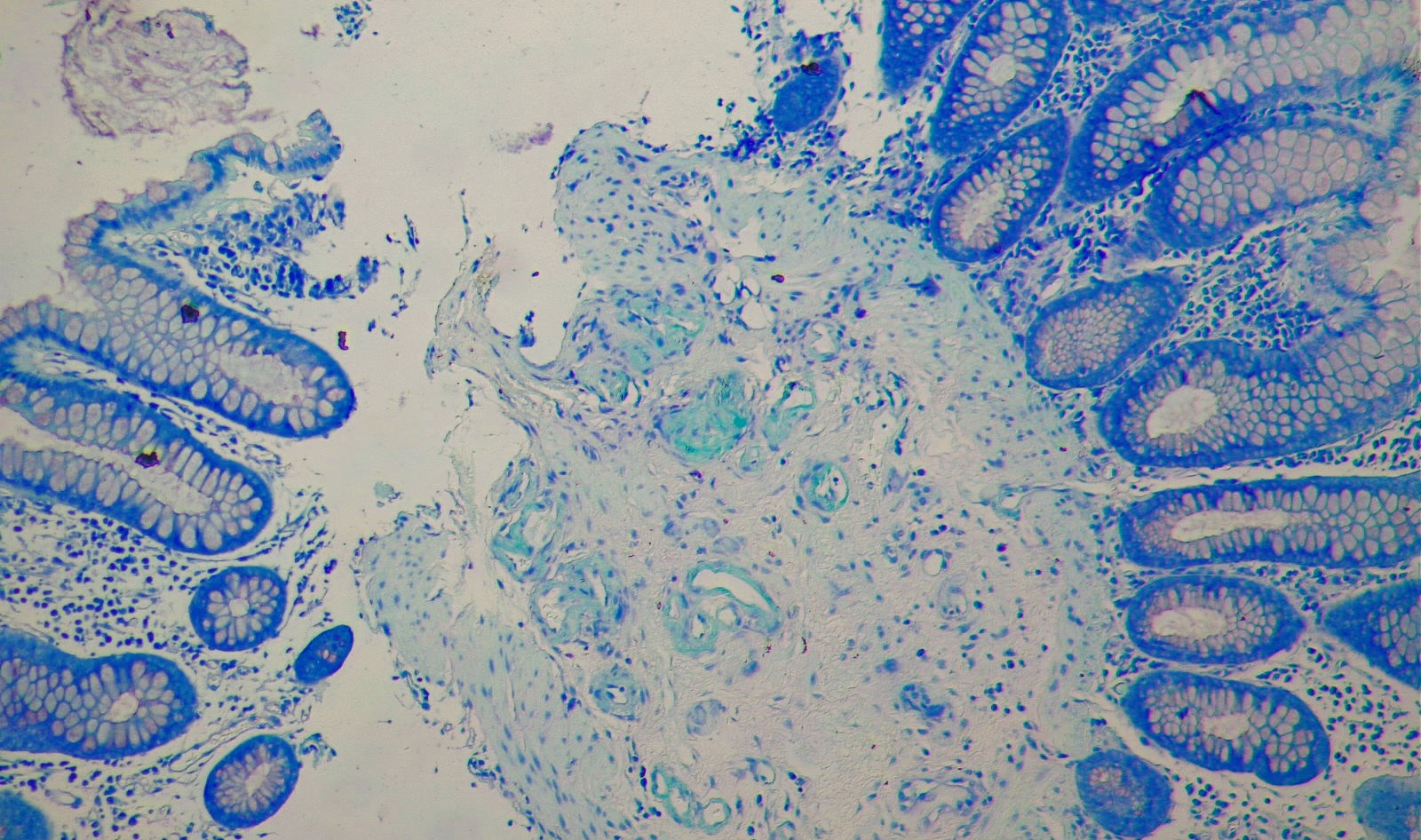
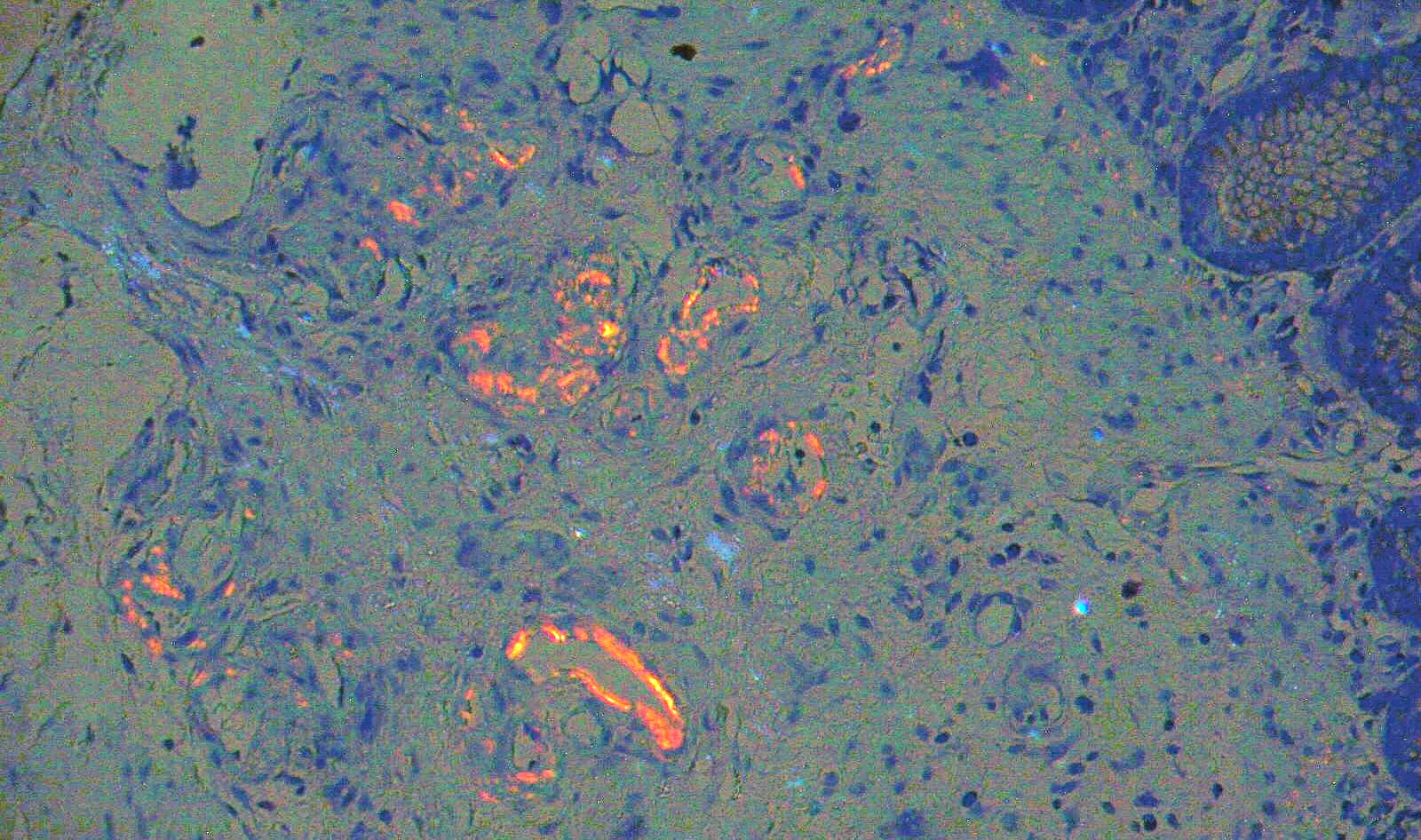
The biopsy samples taken from the colonic mucosa revealed the presence of chronic inflammation, non-diffuse, non-granulomatous, ulcerative, which could be indicative of an inflammatory disease affecting the colon. One of the fragments, with preserved crypts architecture and inflammatory elements within physiological limits, also presents in the submucosa blood pools with the wall including homogeneous hyaline deposits, birefringent green in polarized light (Congo red) , tipically for colonic amyloidosis (Fig.5-9)
Diagnostic :
Colonic amyloidosis.
Discussion :
Gastrointestinal amyloidosis (GIA), a protein deposition disorder, represents a complex common pathway with multiple etiologies and presentations. It represents a significant diagnostic and treatment challenge. The disease results from the deposition of insoluble extracellular protein fragments that have been rendered resistant to digestion. GIA can be acquired or genetic, and most commonly results from chronic inflammatory disorders (AA amyloidosis), hematologic malignancy (AL amyloidosis), and end-stage renal disease (Beta-2 amyloidosis). The diagnosis is based on pathologic examination of the affected tissue, with classic green birefringence under polarized light.
Within the GI tract, amyloid deposition occurs in the muscularis mucosae, within close proximity to vessels, nerves, and nerve plexuses [1]. This deposition increases the frailty of blood vessels, hinders intrinsic peristalsis and decreases the compliance of the gut wall [2]. These mechanisms combined are likely responsible for the symptomatology seen in GI amyloidosis
References :
- Kaiserling E, Krober S. Massive intestinal hemorrhage associated with intestinal amyloidosis. An investigation of underlying pathologic processes. Gen Diagn Pathol. 1995;141:147–154.
- Hirschfield GM. Amyloidosis: a clinico-pathophysiological synopsis. . Semin Cell Dev Biol. 2004;15:39–44.