See other cases
Achalasia: Endoscopic Treatment (POEM)
History :
A 65‑year‑old hypertensive female patient, known with achalasia, with multiple previous balloon dilations (Rigiflex II – 30 mm) and a surgical history 3 years earlier (anterior Heller myotomy with Nissen fundoplication), was admitted for endoscopic treatment of recurrent achalasia. She reported dysphagia for solids and liquids, approximately 9 kg weight loss over the past 6 months, regurgitation, and occasional retrosternal pain.
Clinical & biological :
The patient presented with a mediocre general condition, underweight, hemodynamically and respiratory stable. The abdomen was soft, without signs of peritoneal irritation.
Barium swallow
A markedly dilated esophagus with upstream stasis and a filiform passage of contrast at the esophagogastric junction. At 7 minutes after ingestion, the height of the contrast column measured approximately 10 cm.
Esophageal Manometry
Lower esophageal sphincter pressure: 46 mmHg, with IRP 22.
Aperistaltic esophagus with normal intraluminal pressures, consistent with Type II achalasia.
Eckardt Score: 7
Imaging :
Endoscopic Treatment
The procedure was performed under general anesthesia with the patient in the supine position. A liquid diet was maintained for 72 hours pre‑procedure.
Upper Digestive Endoscopy
- Esophagus: markedly dilated lumen with sigmoid configuration; Z‑line at 38 cm from the incisors; difficult passage of the endoscope into the stomach.
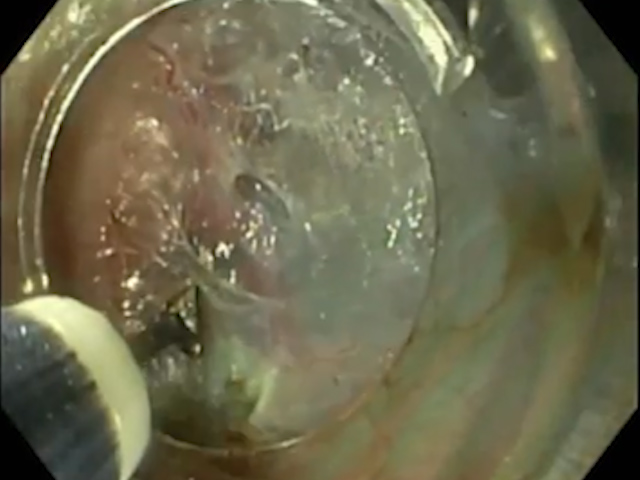
- At 28 cm from the incisors, submucosal injection of saline mixed with methylene blue was performed on the posterior esophageal wall, achieving adequate lifting (Fig. 1).
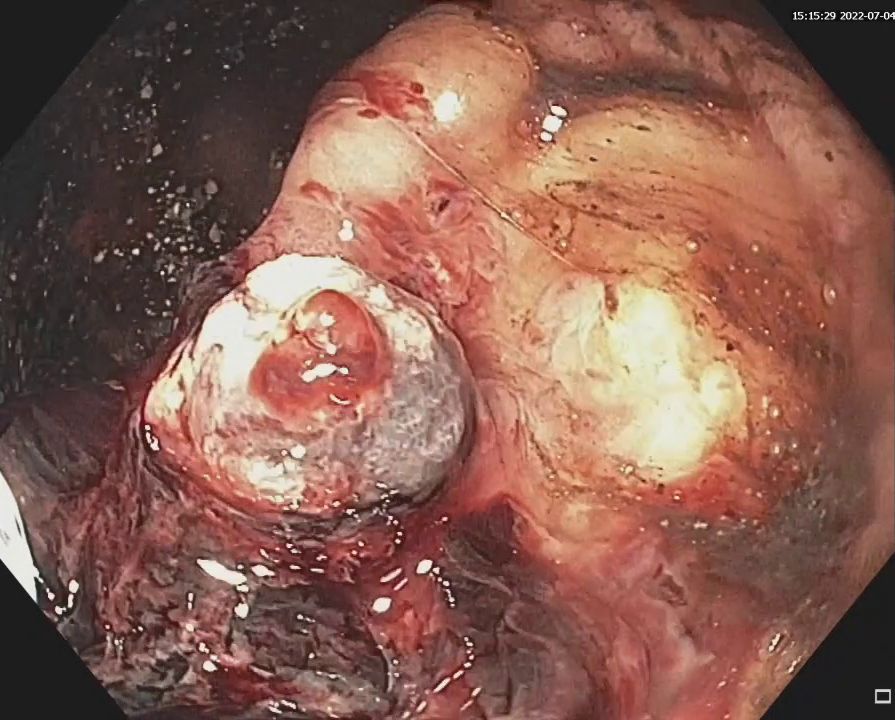
- A longitudinal mucosal incision was made using a triangle knife with cutting current, followed by additional submucosal injection of methylene blue (Fig. 2).
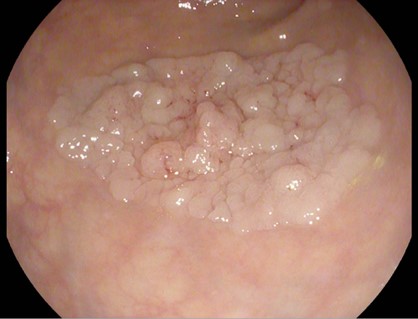
- The submucosal layer was dissected using coagulation current, with coagulation of visible vessels, creating a submucosal tunnel up to 41 cm from the incisors (Fig. 3).
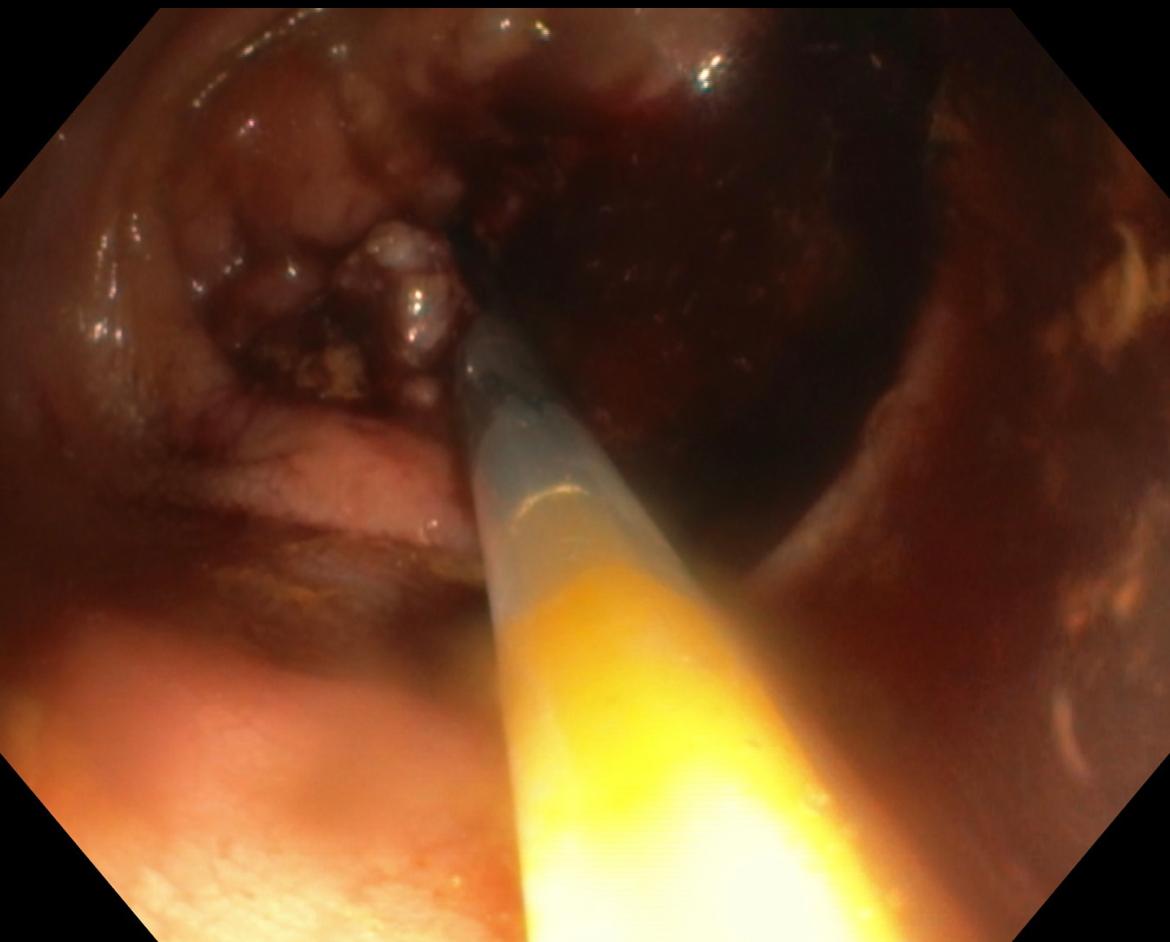
- Myotomy of the circular and longitudinal muscle fibers was performed using a TT knife, from 31 cm to 41 cm from the incisors (Fig. 4).
- The mucosal defect corresponding to the tunnel entry site was closed with seven TTS clips (17 mm opening), the first clip applied approximately 2 cm below the distal end of the mucosal incision (Fig. 5).
Post‑procedural Contrast Study (24 hours after POEM)
Upper digestive contrast study : dilated esophagus without fistulous tracts; free passage of contrast through the esophagogastric junction without stasis.
Clinical Evolution : At 4‑week follow‑up, the patient showed complete resolution of dysphagia, regurgitation, and retrosternal pain.
Diagnostic :
Recurrent, previously operated Type II achalasia
Discussion :
Achalasia is an esophageal motility disorder of unknown etiology, characterized by degeneration of the myenteric plexus, resulting in impaired relaxation of the esophagogastric junction and loss of esophageal peristalsis.
Dysphagia, regurgitation, and retrosternal pain significantly reduce quality of life and limit oral intake. Malnutrition and dehydration are the main contributors to clinical and biological deterioration.
The POEM technique involves:
- Mucosal incision after prior injection of 10 ml saline with methylene blue.
- The incision is typically made ~10 cm above the esophagogastric junction, either on the posterior or anterior esophageal wall.
- Entry into the submucosal space, followed by submucosal dissection and coagulation of submucosal vessels using a coagrasper.
- Continued submucosal dissection down to the esophagogastric junction, followed by gastric submucosal dissection over approximately 3 cm.
- After completing the eso‑gastric tunnel, myotomy of the circular muscle fibers is initiated, with optional extension to longitudinal fibers.
- Myotomy begins approximately 2–3 cm below the mucosal incision.
- Finally, the mucosal entry site is closed with TTS clips.
Conclusion :
Peroral Endoscopic Myotomy (POEM) is an established therapeutic option for achalasia, even for recurrent cases after pneumatic dilation or surgical intervention (Heller myotomy + Nissen fundoplication).
References :
- Roberto de Sire, Antonio Copogreco, Cesare Hassan, Alessandro Repici, Roberto Maselli. Per oral endoscopic myotomy for achalasia. Best Pract Res Clin Gastroenterol. 2024 Aug, 71-101930
- Vamshek Srinivasan, Eric D Shah. Mini-review: Tailored per-oral endoscopic myotomy for type III achalasia. Neurogastroenterol Motil. 2023 Dec, 35 (12), e14700
- Rintaro Hashimoto, Haruhiro Inoue, Yuto Shimamura, Atsushi Sakuraba, Yutaka Tomizawa. Per oral endoscopic myotomy as salvage therapy in patients with achalasia refractory to endoscopic or surgical therapy is technically feasible and safe- systematic review and meta-analysis. Dig Endoscopy. 2020 Nov, 32 (7)- 1042-1049